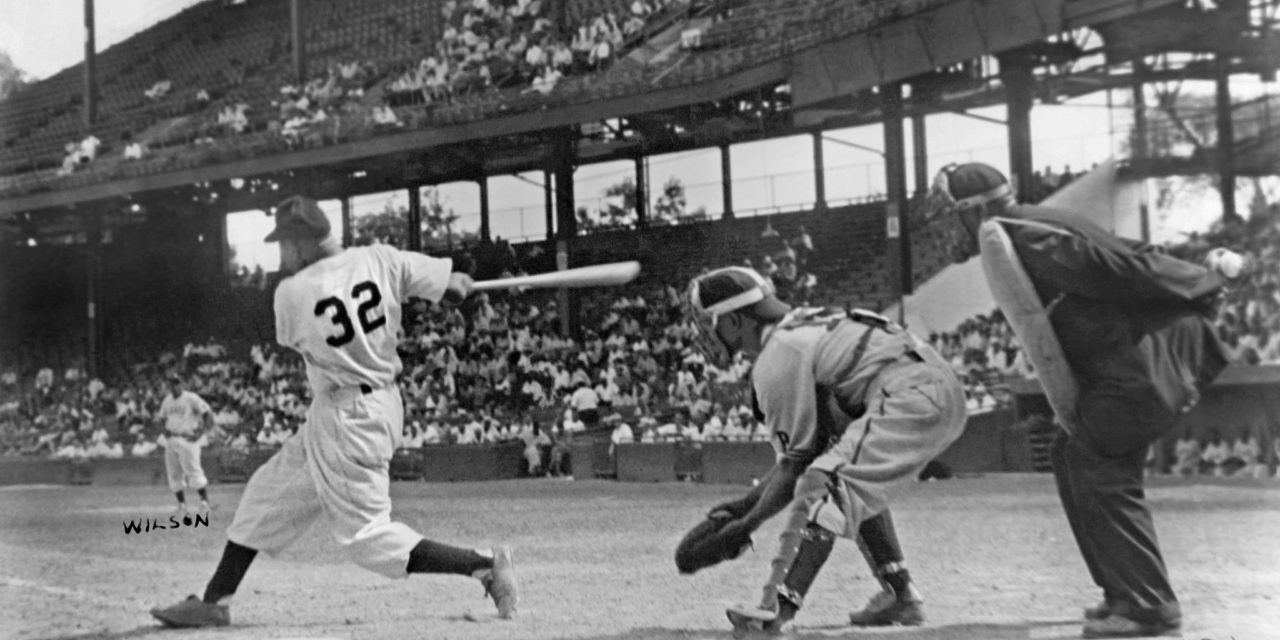
“Baseball’s Unappreciated Power Duo,” the headline on Robert O’Connell’s New York Times story March 27, referred to Josh Gibson and Buck Leonard. The piece begins:
“Baseball’s great power partnerships range from the foundational (Babe Ruth and Lou Gehrig) to the quintessential (Willie Mays and Willie McCovey)… Yet one deserving pair often remains overlooked in these discussions. In the 1930s and ’40s, catcher Josh Gibson and first baseman Buck Leonard anchored one of the most potent lineups in baseball history, but they did so for the Homestead Grays of the Negro leagues.”
There is an analogy between the Negro Leagues and the Society of Cannabis Clinicians —the group of doctors who have been monitoring marijuana use by patients for some 20 years. The Times‘ story continues:
“The disgrace of the time, that qualified stars were barred from the Major League Baseball because of their race, echoes now as a statistical frustration. While their white contemporaries enjoyed M.L.B.’s tidy schedules and scrupulous statistics-keeping, the black players of the early 20th century made do with a mixture of official and unofficial contests across borders of league and nation. The numbers that resulted are slapdash and incomplete…”
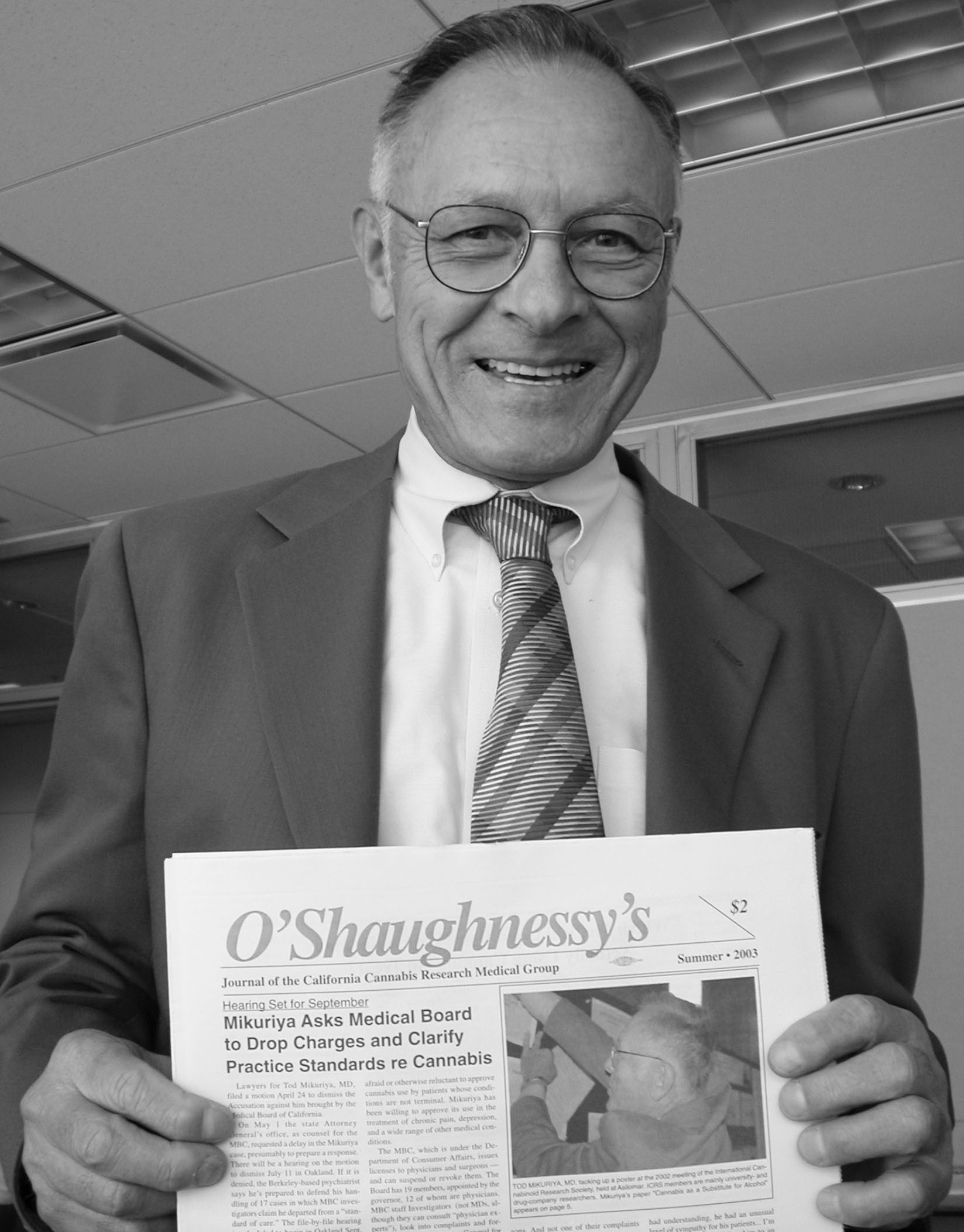
Tod Mikuriya, MD (1934-2007), was the foremost cannabis clinician in the world, but his findings and those of his colleagues were generally ignored by the medical establishment. Mikuriya’s study of the pre-prohibition medical literature led him to conclude that marijuana was useful in treating a wide range of conditions. In the early 1990s his interviews with members of the San Francisco Cannabis Buyers Club confirmed this insight. He inferred that compounds in cannabis were affecting almost every physiological function. He wrote numerous case reports showing that cannabis can be used as a “harm reduction” substitute for alcohol, opioids, and other drugs with adverse side-effects.
Just as the Negro League players “barnstormed” across the country playing semipro teams on many occasions. Mikuriya traveled up and down the state after voters enacted The Compassionate Use Act of 1996, seeing patients at ad hoc clinics. For a few years, he was the only doctor known to readily issue approvals for less-than-grave conditions such as chronic pain and depression. As others began specializing in treating cannabis users, Mikuriya organized them into the California Cannabis Research Medical Group, which became the Society of Cannabis Clinicians (SCC) when doctors from other states began joining.
Mikuriya saw the need for a journal in which cannabis clinicians could share their findings and observations. I helped him launch O’Shaughnessy’s in 2003. He named it after a “personal hero,” William Brooke O’Shaughnessy, the Irish-born, Scottish educated physician sent by the British East India Company to Calcutta in 1839, where he observed doctors using cannabis tinctures to treat epilepsy and other disorders. A paper by O’Shaughnessy in the Provincial Medical Journal in 1843 is considered the introduction of cannabis to Western Medicine.
In 2006, the 10-year point of legalization for medical use in California, Mikuriya surveyed his colleagues in the SCC and published the results in a paper, “Medical Marijuana in California, 1996-2006” (O’Shaughnessy’s, Winter/Spring 2007). The major findings have been confirmed by other studies over the years and this process will likely continue as the federal stranglehold on research weakens.
All the SCC doctors reported in 2006 that pain patients were reducing opioid use —typically by 50%— by adding cannabis to their regimen. This is how Helen Nunberg, MD, worded it: “49% of patients using cannabis for chronic pain were previously prescribed an opioid (such as hydrocodone) by their personal physician.” Many of the SCC doctors’ patients had gotten off opioids entirely
Unusual benefits of cannabis were also reported in the SCC survey. To cite but one example, lowered resistance to graft implantation was reported in a case note by William Toy, MD:
“A 62-year-old man who had a heart transplant from the Stanford program 22 years ago. He apparently is the longest surviving transplant patient in the program. He has been using large doses of cannabis ever since he received the transplant. He is convinced that cannabis not only reduces the side-effects of his anti-rejection drugs, but that it has anti-rejection properties. He feels that he owes his star status in Dr. Shumway’s program to the modulation of his immune system by cannabis.”
O’Connell of the Times describes segregation by Major League Baseball as “the disgrace of the time,” with “qualified stars… barred because of their race.” How should we describe segregation by Major League Medicine? The findings of cannabis clinicians have been barred from “the literature” on grounds more sophisticated than race (a crude, pseudo-scientific concept). The exclusion is based on the “quality of evidence” the cannabis specialists have published
In fact, the intellectual segregation is so strict that the word publish simply doesn’t apply to articles not indexed in Major League Medicine’s official record book, PubMed Central. The survey by Mikuriya et al may have been printed on electrobrite paper and distributed (20,000 copies) by doctors and dispensary operators, but it was not “published.” Nor did I just cite a case note by Dr. Toy, because only material published in “the literature” can be cited. I’m not making this up. The elitist jargon dismisses certain sources of knowledge as second-class. Segregation is built into the language of Capital-S Science.
The National Academy of Sciences, in developing its 2017 Report, The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research, ranked case reports lower than even “low-quality evidence” in terms of credibility. Case reports were simply excluded from consideration. Also excluded were abstracts from conferences and “‘N-of-1’ studies” in which patients serve as their own controls by reporting effects during alternating periods of drug use and abstinence.
O’Connell of the Times explains that meaningful statistical comparisons with Major League Baseball can’t be made because, “Negro leagues teams interspersed their schedules with games against semipro or independent squads; of the 200 or so games they played in a summer, fewer than half were official Negro leagues contests. Statistics and box scores even for those can be hard to track down, compiled as they were not by an official steward of the leagues but by the daily box scores of African-American newspapers like The Chicago Defender and The Pittsburgh Courier.”
This is analogous to noting that Tod Mikuriya and his colleagues used differently worded intake questionnaires and reported their findings in a tabloid. Why disregard the clear pattern they discerned? It’s discrimination disguised as “Rigor.” Pain patients who use cannabis reported cuting back on opioid intake no matter how the doctors phrased the question!
Our nation is now 13 years deeper into a terrible opioid epidemic. Studies are beginning to appear in the literature that echo the findings of Mikuriya and his colleagues: cannabis use can reduce opioid consumption. Other academic studies have echoed other findings by the real-world doctors: cannabis ameliorates a very wide range of symptoms. Years of clinical trials will ensue, and in the end, every finding of benefit reported by the SCC doctors will be confirmed. The neo-prohibitionists’ success is measured in how long they can delay the inevitable revelations.