Dr. Peter Grinspoon tweeted July 23, “”I just had a patient respond spectacularly to small-ish dose of cannabis with complete resolution of restless leg syndrome (RLS) and virtually no side effects. More evidence of cannabis efficacy in restless legs syndrome.” (He uses both singular leg and plural legs, as does the medical literature. The trend seems to be towards the plural.)
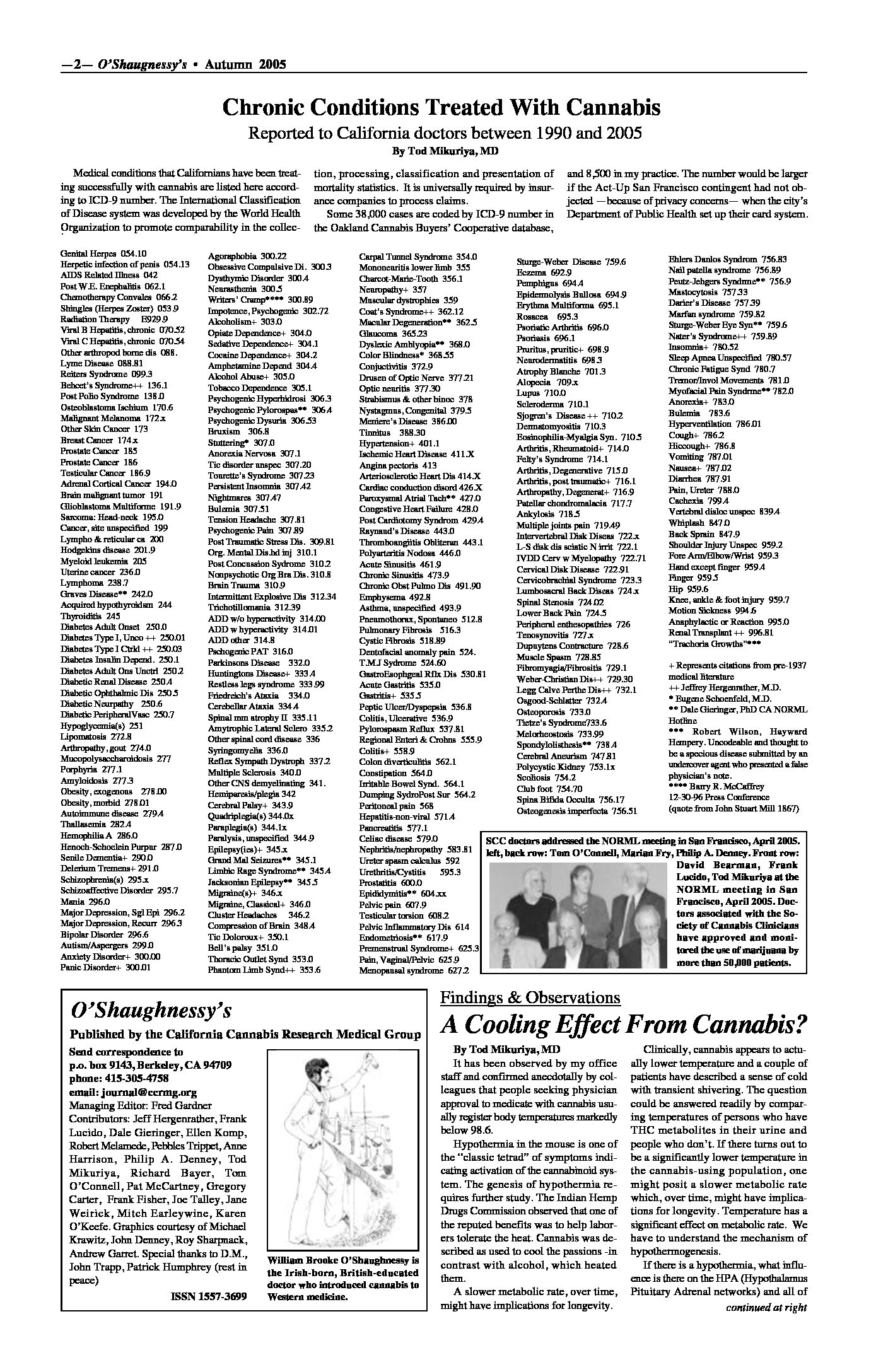
Restless Leg Syndrome was one of the numerous medical conditions for which Dr. Tod Mikuriya’s patients reported using cannabis effectively. In the Spring 2005 issue of O’Shaughnessy’s, drawing on his extensive patient files and the slim pre-prohibition medical literature, Mikuriya published a master list of conditions for which cannabis had been shown to provide relief. (RLS is 333.99 in the graphic.) At an early meeting of the Society of Cannabis Clinicians, Mikuriya arranged for a speaker to explain and advocate use of ICD-9 coding as an aid to aggregating data.
I had never heard of the disorder, which Mikuriya described as “surprisingly widespread.” According to the National Institutes of Health, RLS “causes unpleasant or uncomfortable sensations in the legs and an irresistible urge to move them. Symptoms commonly occur in the late afternoon or evening hours, and are often most severe at night when a person is resting, such as sitting or lying in bed. They also may occur when someone is inactive and sitting for extended periods (for example, when taking a trip by plane or watching a movie). Since symptoms can increase in severity during the night, it could become difficult to fall asleep or return to sleep after waking up. Moving the legs or walking typically relieves the discomfort but the sensations often recur once the movement stops. RLS is classified as a sleep disorder since the symptoms are triggered by resting and attempting to sleep, and as a movement disorder, since people are forced to move their legs in order to relieve symptoms. It is, however, best characterized as a neurological sensory disorder with symptoms that are produced from within the brain itself.”
The sad reality is that the clinical evidence developed by Mikuriya and his SCC colleagues has been essentially ignored by capital-M Medicine. (See Evidence-Based Medicine vs Medical Cannabis and Clinicians’ Input Sytematically Ignored.) Mikuriya called the process “a stall in the name of science.” It’s revealing that in 2021, the admirable Dr. Grinspoon considers it news worth sharing that cannabis can prevent and/or relieve Restless Leg Syndrome.
By deeming that only Placebo-Controlled, Randomized Clinical Trials can establish medical efficacy, neo-prohibitionists have, over the years, denied millions of Americans access to a medicine whose cost is much lower and side effects less ominous than the alternatives provided by Big Pharma. WebMD estimates that “7-10 percent of the U.S. population may have RLS” and describes the symptoms as ranging from mild to severe. That adds up to countless years of avoidable pain and suffering.
In 2008 the FDA approved a dopamine agonist called ripinirole for RLS (and Parkinson’s), which was sold as “Requip” by GlaxoSmithKline. The mechanism of action had not been clearly elucidated. Common side effects, according to RxList.com, include drowsiness, dizziness, weakness; headache, confusion, hallucinations; increased blood pressure (severe headache, pounding in your neck or ears, nosebleed, irregular heartbeats); nausea, vomiting, upset stomach, constipation; flu symptoms (fever, chills, body aches); sudden muscle movements; increased sweating; or swelling in your legs or feet.
The assault on the neoprobe citadel —PubMed Central— is continuing apace. The journal Sleep and Breathing published a short communication entitled “More evidence of cannabis efficacy in restless legs syndrome” by Imad Ghorayeb, a researcher at the University of Bordeaux, in December 2019. The abstract concludes with a call for robust clinical trials.
Restless legs syndrome (RLS) is one of the most disabling and sometimes painful sensorimotor ailment of the nervous system that has only in recent years become more widely accepted as a clinical disorder with its own distinct features. Usually, symptoms respond well to dopamine agonists, anticonvulsants, or opiates, but still a subset of patients remains refractory to medical therapy and/or reports serious side effects. Recently, patients’ statement of a remarkable and total remission of RLS symptoms following cannabis use has been reported. Here, we confirm and extend these findings to more patients with RLS. The antinociceptive effect of marijuana has been documented in many painful neurological conditions, and the potential benefit of cannabis use in patients with refractory RLS should therefore be questioned by robust clinical trials.
In the days and months and years to come, as the medical establishment reluctantly but inevitably yields to real-world pressure, the long-delayed clinical trials will be conducted. The conditions identified by SCC doctors and their patients as amenable to treatment by cannabis will inevitably make their way into “the literature.” There is no way to measure the cost and suffering Neoprohibition has caused and continues to cause.