Cannabis Via ‘Telehealth’
By Fred Gardner March 29, 2016 The Medical Board of California is now looser than the Society of Cannabis Clinicians when it comes to doctors authorizing cannabis use by patients. SCC practice standards assert that the initial doctor-patient interaction should be in person. The medical board has no such requirement. In its final meeting of 2014, the MBC adopted a policy stating:
Telehealth (previously called telemedicine) is seen as a tool in medical practice, not a separate form of medicine. There are no legal prohibitions to using technology in the practice of medicine, as long as the practice is done by a California licensed physician. Telehealth is not a telephone conversation, email/instant messaging conversation, or fax; it typically involves the application of videoconferencing or store and forward technology to provide or support health care delivery.
The standard of care is the same whether the patient is seen in-person, through telehealth or other methods of electronically enabled health care. Physicians need not reside in California, as long as they have a valid, current California license.
As of January, 2016, 48 states and the District of Columbia provide Medicaid payment for telehealth services. Only California and Nevada allow doctors to issue medical cannabis evaluations without an in-person evaluation.
Coordinating calls
Perry Solomon, MD, who had spent more than 20 years as an anesthesiologist, agreed to co-found HelloMD in April, 2015. He joined the SCC and he credits the SCC’s CME course with providing his introduction to the field of Cannabis-based Medicine. All the doctors he hires are required to take the 12-module program. At the December SCC meeting, Solomon informally questioned Jeffrey Hergenrather, MD, about the basis for the SCC’s position on in-person initial visits. Hergenrather noted that he, Frank Lucido, MD, and other SCC docs had, on occasion, detected serious medical problems that they almost certainly would have missed online.
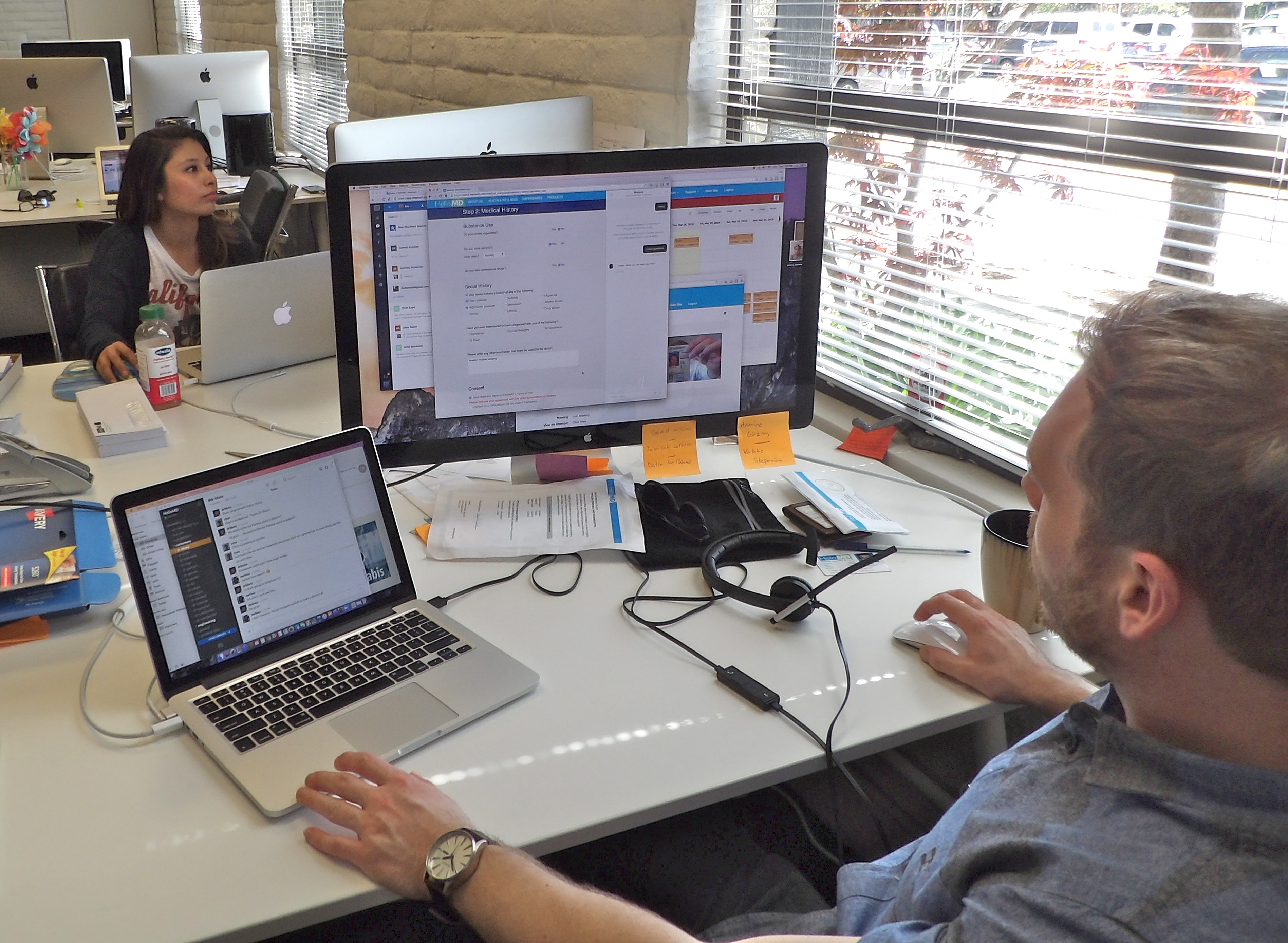
Last week I visited HelloMD headquarters in San Rafael —a clean, well-lighted space that could have been an ad for Apple. Two customer service representatives were coordinating videoconferences between patients and doctors, and fielding inquiries. The fee for an evaluation or a renewal is $49.
“The doctor’s interaction with each patient is usually 10-15 minutes,” Solomon said. “We usually have three doctors online from 10 a.m. to 7 p.m. at remote locations. Zoom is our televideo conference because they’re HIPPA compliant —they can’t be hacked. Everything is in The Cloud… If a patient is from out of California we have to turn them down. We have plans to expand to other states. We get hundreds of calls a week from people in other states. There’s such a demand for medical cannabis!”
Asked if HelloMD helped patients develop a treatment plan, Solomon said, “To a degree. If someone says ‘I’m very anxious,’ we might suggest an Indica strain. We don’t recommend specific brands. There is no advertising on our site, but there are some brands we’re trying to familiarize our physicians with. For example, Foria Relief for menstrual cramps and Foria Pleasure for female sexuality.”
We proceeded to a conference room and were joined by Mark Hadfield, a 40-something tech entrepreneur who, with his wife, Pamela Hadfield, had launched the company —his fourth, her first. Her background is in user interface and design, and the sleek HelloMD site reflects her expertise.
“We started a service for traditional health care, not for cannabis,” Hadfield recounted. “We built a platform to connect patients to doctors on smart phones. That market was big but increasingly competitive. My wife had started using cannabis products for migraines and her experience getting a card was not ideal —which gave us the thought that we can we do telehealth for cannabis. So we decided to pivot. At that time we had 150 doctors on board the platform: neurologists, oncologists, surgeons. But when we said ‘We’re going to do cannabis,’ all 150 said goodbye.”
Solomon, who met the Hadfields through a mutual friend, got his MD from Columbia in 1981. He spent much of his career at San Ramon Regional Medical Center, where he helped start the Anesthesia Department. Although he says he had “done the usual experimentation at college,” Solomon knew little about cannabis as medicine when Mark Hadfield asked him to join HelloMD. Some quick research convinced him that cannabis had a very benign safety profile. Feedback from patients would soon convince him that it was indeed extremely beneficial.

Perry Solomon, MD
The clincher, he says, was a meeting of the medical marijuana club at Rossmoor, a retirement community in Walnut Creek. “It was an overflow crowd —a hundred people. More than 80 percent were using medic
inal cannabis for pain. ‘I don’t have arthritic pain…’ ‘I can walk around…’ I don’t have constipation…’ That’s when I knew it was for real. There are millions of people with chronic pain! Now you have the CDC saying doctors shouldn’t prescribe opioids for chronic pain. Cannabis is the alternative.”
There are now 25 physicians associated with HelloMD, all with licenses to practice in California, though some reside in other states. T0 recruit them, Solomon says, “At first we used a company to send us resumes of physicians who were looking for freelance work. I’d review them, do the usual search of their medical licenses, etc. Ones that passed and seemed like a match to us, I would do a Zoom interview with them for about 30 minutes to gauge their interest, knowledge and time commitment, as well as to make sure they were able to communicate with patients in a professional manner and location. Many came from a cannabis background and wanted to change the way that they were seeing patients. Some had been with brick-and-mortar evaluation centers and wanted a more convenient way to see patients. Some had just gotten interested in medicinal cannabis. Everyone, regardless of their baseline knowledge, needs to take the SCC Cannabis course. I encourage all of them to join the SCC for the educational opportunities. We have active communication with all our physicians in terms of education, new products, etc.
“Once we had the first several on board, the subsequent physicians would ‘shadow’ the existing docs for an hour or so to see the patient flow, type of patients, etc. All this is done, of course, after asking the patient if we had their permission. If they, and we, felt that it was a match, we would proceed.
“Now,” he adds, thanks to a few paragraphs in a New York Times article last November, “we are being solicited by physicians themselves from all over the country. Some have their California license already, and so
me would obtain it.” Solomon says no complaints of any kind have been brought to his attention. “We’d like to be able to help kids,” he says. “Right now we’re not treating people under 18. There are a lot of time-consuming logistical problems. Dealing with parents can be complicated. We refer them to CannaKids in LA. or other organizations set up for younger patients needing medical cannabis”
Hadfield put in: “If you live in a city where you can safely go to a nearby doctor, that’s great. But we have all of California. And even if you live in San Francisco, you may have to drive to a bad area of town and park and wait… You don’t know who you’re going to see… People
who have never gotten an approval to use cannabis and probably wouldn’t participate, now feel comfortable doing so because they can do so from the privacy of their own home and they can get delivery as well, they don’t have to visit a dispensary.

Tech entrepreneur Mark Hatfield
HelloMD is planning to survey patients on the extent to which cannabis has enabled them to reduce or eliminate opioid consumption. I’ll lay anybody 2-to-1 odds that the average reduction will be around 50%. That’s what SCC docs have reported over the years, and as Tod Mikuriya used to say, “Neither cannabis nor human physiology have changed that much over time.”
Hadfield is ambitious. “Our plan is to expand nationally and even internationally. We have millions of people coming into the industry who are confused. They haven’t tried cannabis and they have medical issues that their traditional doctor is not equipped to talk to them about, or which they’d rather not discuss with their traditional doctor. We want to make those connections between new patients with questions and the medical community —whether they be doctors or nurses or product specialists or bud tenders— who have the answers. The videoconference is just one way to facilitate that. There’s text-based exchanges, webinars, educational materials, et cetera. From the doctor’s perspective, the more they participate the more they propel their own image as an expert. We have a patient community of 35,000 that is doubling every two months.”
Competitors such as Meadow and PrestoDoctor are coming into the field, and Hadfield keeps seeking an edge. “As we expand,” he says, “we are not committed to telehealth. We see ourselves as the first contact with the patient. If it requires an in-person visit, we can facilitate that as well.”
Hadfield and Solomon recognize that applicants fall into two broad classes: those seeking legal protection (many are already using medical cannabis), and those seeking a serious treatment plan. Maybe there could be synergy with the SCC in connection with the latter.