
La Jolla Pain Management Specialist Nancy Sajben, MD, appreciates the “Agreement” that the Medical Board of California intends to provide to physicians for signing by cannabis-using patients. Sajben writes:
“These agreements are quite traditional when considering prescription opioids for pain. We cannot assume patients understand safe use.
“It covers the bases specified by law and would reassure many of the patients I see who are afraid to use it and allows some legal protection to an MD.
“There is no substitute for regular followup as required for monthly opioid prescriptions, but that is not usually possible with prescriptions for MMJ.”
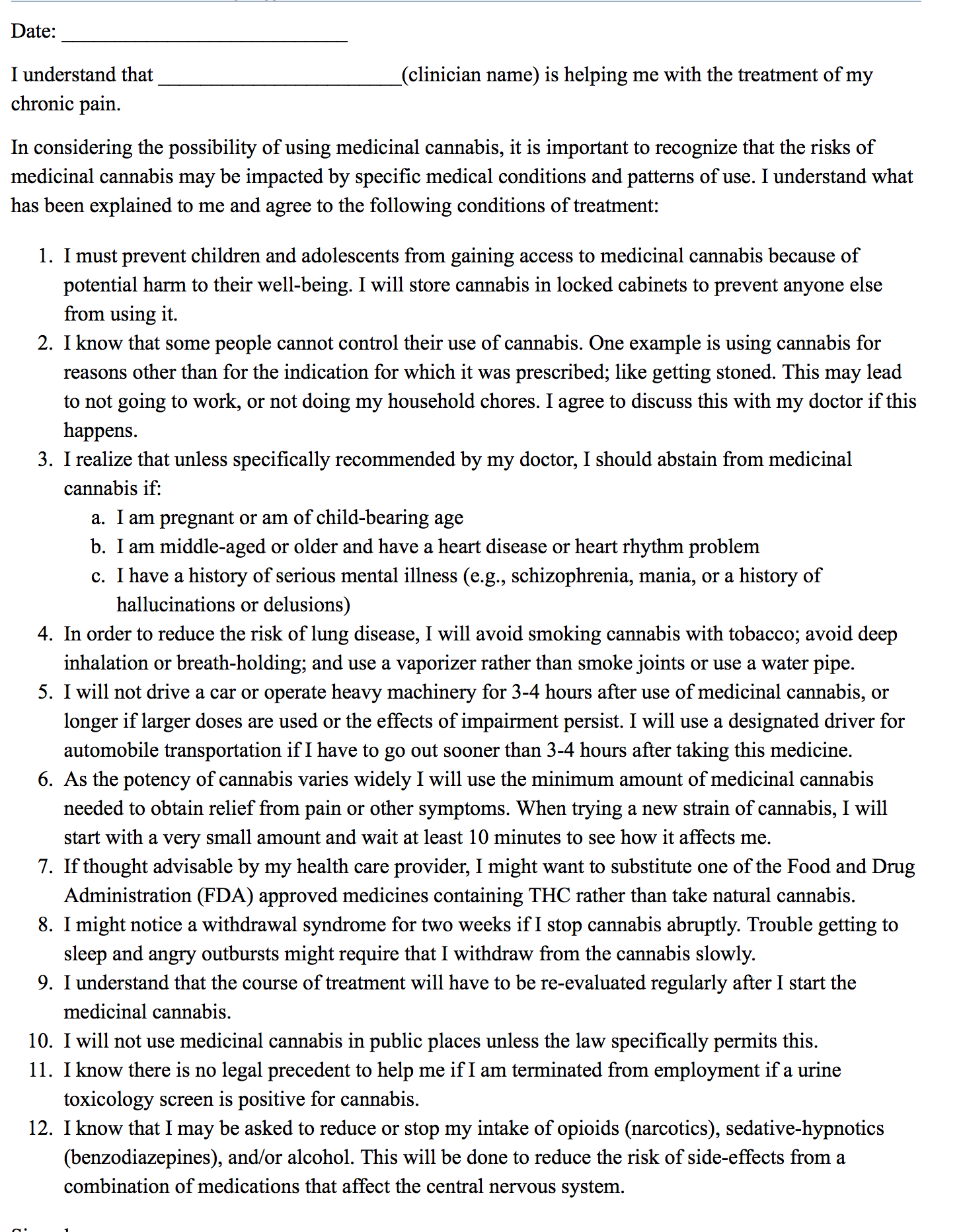
Other members of the Society of Cannabis Clinicians are voicing strong objections to the Agreement, which they consider excessively fear-inducing. It was published in the Clinical Journal of Pain: December 2015, the culmination of a paper justifying its 12 Tenets.
The following points have been deemed particularly objectionable by SCCers:
• 3. “I should abstain from medical cannabis if I am pregnant or am of child-bearing age.” No young woman should use medical marijuana?
• 5. “I will not drive a car or operate heavy machinery for 3-4 hours after use of medicinal cannabis, or longer if larger doses are used.” Imagine similar advice to alcohol drinkers!
• 6. “When trying a new strain of cannabis, I will start with a very small amount and wait at least 10 minutes to see how it affects me.” One or two minutes after inhalation is plenty, and 10 minutes after ingestion is not enough. In any case, all cannabis in California will be labeled for potency once regulations kick in.• 7. “If thought advisable by my health care provider, I might want to substitute one of the FDA approved medicines containing THC rather than take natural cannabis.” Who but the pharmaceutical manufacturers want to encourage this substitution?• 10. “I will not use medicinal cannabis in public places unless the law specifically permits this.” Homeless patients have no private place to use cannabis. This is a matter for law enforcement, not clinicians.
• 11. “I know there is no legal precedent to help me if I am terminated from employment if a urine tox screen is positive for cannabis.” Several states do have legal precedents protecting employees who are medical users. California law might change.
• 12. “I know that I may be asked to reduce or stop my intake of opioids, sedative-hypnotics and/or alcohol. This will be done to reduce the risk of side-effects from a combination of medications that affect the CNS” This is positively harmful. It encourages discrimination against marijuana use by opiate users and there is no good scientific evidence supporting it.
Principal author Brad Wilsey, MD, defended the utility of the Agreement at a recent meeting of the med board’s Cannabis Task Force.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4417655/
One of the Agreement’s co-authors, Igor Grant, MD, is director of the Center for Medical Cannabis Research, whose input was sought by the Medical Board’s Cannabis Task Force in drafting Guidelines for Physicians who Recommend Cannabis. The guidelines will be discussed, possibly revised, and almost certainly adopted when the full board meets in San Diego October 26-27. Executive Director Kimberly Kirchmeyer says the CMCR Guidelines will be attached to the guidelines as “a sample.”
Treating alcoholism by cannabis substitution creates a different doctor-patient relationship. Patients seek out the physician to confer legitimacy on what they are doing or are about to do. My most important service is to end their criminal status —Aeschlapian protection from the criminal justice system— which often brings an expression of relief. An alliance is created that promotes candor and trust. The physician is permitted to act as a coach —an enabler in a positive sense.
As enumerated by patients, the benefits can be profound: self-respect is enhanced; family and community relationships improve; a sense of social alienation diminishes. A recurrent theme at follow-up visits is the developing sense of freedom as cannabis use replaces the intoxication-withdrawal-recovery cycle —freedom to look into the future and plan instead of being mired in a dysfunctional past and present; freedom from crisis and distraction, making possible pursuit of long-term goals that include family and community.


{kind=link}