By Jeffrey Hergenrather, MD
Letter to a colleague, November 7, 2019 I wanted to send to you a few things that you may or may not have seen about glaucoma and cannabis. As you check out these sources of information we’ll agree that the interpretation of the information depends upon your viewpoint. So, for myself as a physician in California where cannabis can be recommended by a physician or used without medical approval by any adult, my perspective is a bit different from yours (with both the Israeli medical profession and the government looking over your shoulder)’.
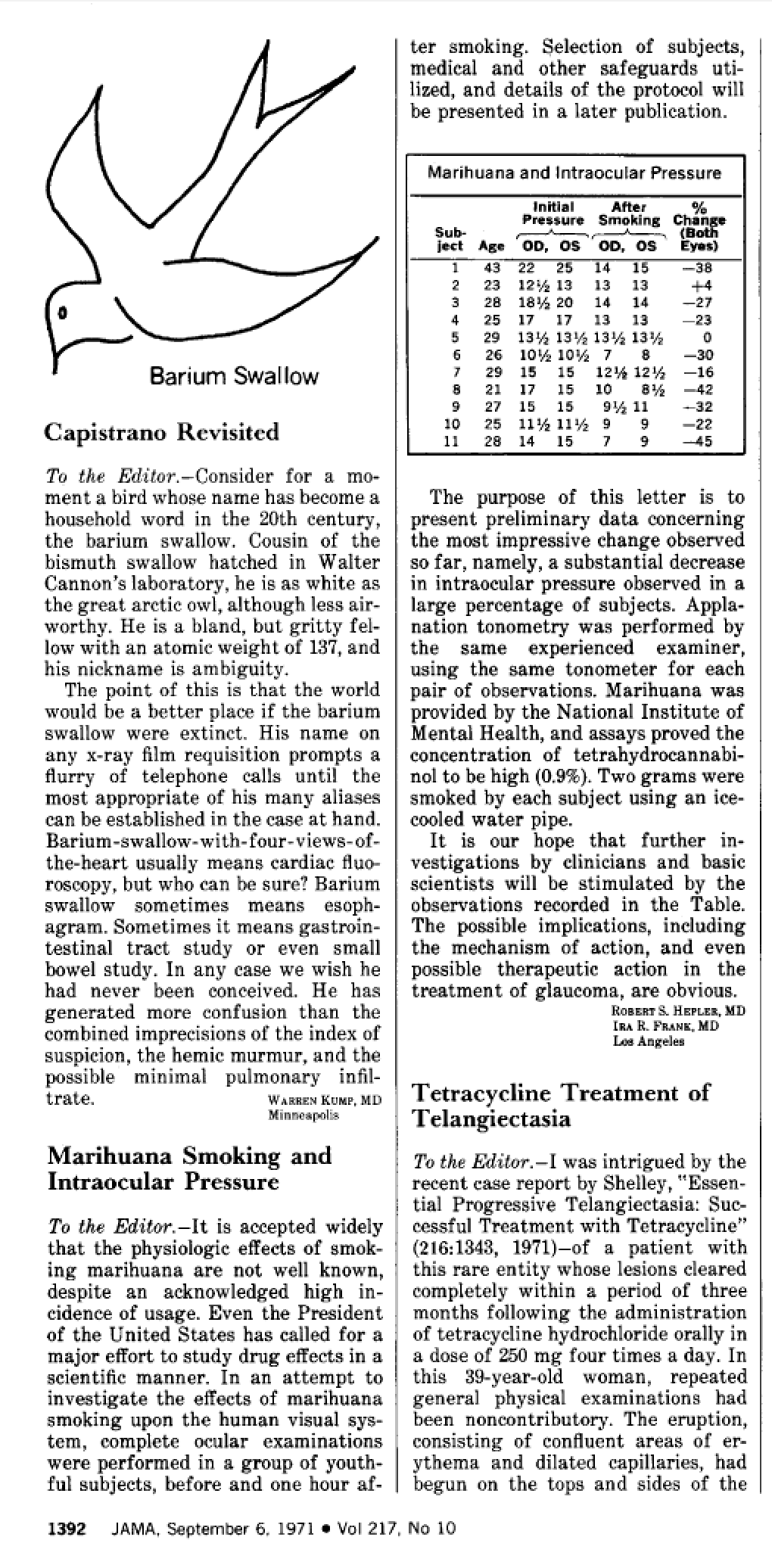
First is the 1971 JAMA letter to the editor by Dr. Robert Hepler: “Marihuana Smoking and Intraocular Pressure.”
Next is a chronological string of documents and their sources from 1992 until 2014. Following the list are my critiques of the documents. Bold lettering has been added by me.
1. American Academy of Ophthalmology. Information About Eye Care: The Use of Marijuana in the Treatment of Glaucoma. San Francisco: American Academy of Ophthalmology, 1992.
1992 Statement from the AAO, American Academy of Ophthalmology concluded: there was no scientifically verifiable evidence that the use of marijuana is safe and effective in the treatment of glaucoma.
‘The Academy could not support proposed legislation to transfer marijuana from Schedule I to Schedule II of the Controlled Substances Act in order to permit its use in treating glaucoma’.
2. National Eye Institute, National Institutes of Health. NEI Statement – The Use of Marijuana for Glaucoma. Bethesda: NEI/NIH, February 18, 1997.
1997, the NEI (National Eye Institute of the NIH) concluded that “none of these studies demonstrated that marijuana–or any of its components–could safely and effectively lower IOP any more than a variety of drugs on the market”
[the NEI sponsored research studies on the use of marijuana from 1978 to 1984]
3. Kaufman PL. Marijuana and glaucoma. Arch Ophthalmol 1998; 116:1512-3. [Comment on Arch Ophthalmol 1998; 116:1433-7]
1998 an editorial in the Archives of Ophthalmology noted, “In summary, decreased blood pressure, decreased optic nerve blood flow and short duration of the IOP-lowering effect are significant actual and potential problems with marijuana, in addition to the psychotropic effects”
4. Plange N, et.al. Dronabinol and retinal hemodynamics in humans. Am J Ophthalmol. 2007 Jan;143(1):173-4. Bethesda: NEI/NIH, February 18, 1997
2007 THC (7.5 mg Dronabinol) orally, is shown to improve blood circulation in the retina and reduce intraocular pressure.
5. Marijuana and Medicine: Assessing the Science Base, Institute of Medicine, 1999, Editors Joy, JE, Watson, SJ Jr., and Benson, John A Jr
1999 Institute of Medicine report concluded that although IOP can be reduced by using cannabinoids and marijuana, they opine “… the effect is too short lived and requires too high doses, and there are too many side effects to recommend lifelong use in the treatment of glaucoma. The potential harmful effects of chronic marijuana smoking outweigh its modest benefits in the treatment of glaucoma. Clinical studies on the effects of smoked marijuana are unlikely to result in improved treatment for glaucoma.”(59)
The co-author, John A. Benson concluded that “we did not find compelling evidence that marijuana should be used to treat glaucoma.”
6. AAO Complementary Therapy Task Force, Hoskins Center for Quality Eye Care
Glaucoma, Jun 2014, Marijuana in the Treatment of Glaucoma CTA – 2014
Base, Institute of Medicine, 1999, Editors Joy, JE, Watson, SJ Jr., and Benson, John A Jr
2014 The American Academy of Ophthalmology (AAO) (54) recommends use of medications including topical miotics, beta adrenergic blockers, epinephrine derivatives, carbonic anhydrase inhibitors, alpha adrenergic agonists, and prostaglandin analogs as well as surgical treatments, such as laser trabeculoectomy, drainage devices, and cyclodestruction which have been used effectively to lower IOP.
Critique:
It is acknowledged that if people are ‘growing and using their own marijuana’, they may achieve an adequate treatment of elevated IOP and neuroprotection to the optic nerve. But the thrust of both the AAO and NEI have been to thwart any consideration of cannabis as an alternative to conventional ophthalmological care. Why? Could it be because cannabis use would reduce the need for conventional pharmaceutical and surgical care of glaucoma provided by ophthalmologists?
In the previous 6 citations:
1. ‘There is no scientifically verifiable evidence’, not because studies did not show IOP lowering but because such studies aren’t allowed nor does the AAO accept that it should even be studied.
2. ‘None of these studies demonstrated that marijuana –or any of its components– could safely and effectively lower IOP any more than a variety of drugs on the market’. Here, the NEI/NIH points out that marijuana is lowering pressure no more than the drugs on the market. It is lowering pressure, just not more than the pharmaceuticals.
3. Coming out in 1998 this was, in effect a response to California’s passing the medical use of cannabis in 1996. Other states were legalizing the medical use of cannabis. This editorial was surmising the potential problems of smoked cannabis on retinal artery blood flow, mild lowering of systemic blood pressure, and the short duration of IOP-lowering effect of cannabis without recognizing the prolonged duration of action of ingested cannabinoids that can be designed to limit psychoactivity.
4. In 2007 dronabinol (synthetic THC) was shown to lower IOP and improve retinal blood, flow contradicting the assertions of harm from the Archives of Ophthalmology.
5. Marijuana and Medicine: Assessing the Science Base, from the Institute of Medicine in 1999 attempted to summarize the earlier findings and opinion. Dr. John Benson, one of the authors, sums up the negatives: it is too short lived, requires too high a dosage, and has potential adverse effects. This is nothing more than opinion without a controlled trial of cannabis as a treatment for Glaucoma. Today, with hundreds of cannabis strains available, and numerous methods of administration, the IOM report needs updating.
6. The American Association of Ophthalmologists task force report in 2014 gets right to the crux of the matter: the ophthalmologists don’t want any competition from cannabis to interfere with their treatment modalities of drugs and surgeries. Nobody has even considered possible benefit from the neuroprotective aspects of cannabinoids —which may be as helpful in protecting the optic nerve as the IOP-lowering effects. Again, no research, no competition.
I hope this collection of documents is useful to you. The ophthalmologists I work with in California don’t want to cross the line with their AAO, fearing reprisals from their professional society. They prefer to refer their patients to me for adjunctive treatment with cannabis.
Best wishes,
Jeff