Dennis Peron was the Rosa Parks of the medical marijuana movement, the one who would not move to the back of the bus. Dennis refused to accept that anybody —any cop or DA or judge— could tell him he didn’t have a right to smoke marijuana. “And the right to smoke it means the right to get it,” he would argue, “which means people have to have the right to grow it and sell it.”
Dennis was a Vietnam vet. During the Tet offensive in February, 1968, he had stacked body bags and come out as a gay man. Back in San Francisco at the start of the ’70s he said, “I want to dedicate my life to world peace.” A hippie who meant it. He believed that marijuana was inherently an anti-war drug due to its relaxing effect on the individual and the sharing ritual associated with its use. In the ’ 70s and ’ 80s he was busted for selling pot more than a dozen times. During a raid in 1977 he took an SFPD bullet that splintered his thigh. And after every bust he would resume selling. How the narcs hated him.
Dennis did not fancy being an outlaw, so after the 1977 bust he drafted and collected signatures for an initiative —aptly named ‘W’— whereby the people of San Francisco instructed their law enforcement officials not to press any marijuana-related charges. It carried, and Mayor George Moscone notified the police that possession of an ounce or less should henceforth be ignored. Moscone would soon be assassinated.
As the ’80s ended, Dennis’s longtime companion Jonathan West was dying of AIDS. “Jonathan was taking many prescribed drugs,” Dennis explained, “and there were severe side effects, from nausea to loss of appetite. Marijuana was the only drug that eased his pain and restored his appetite and gave him some moments of dignity in that last year. And of course I had hundreds of friends with AIDS who relied on marijuana for the same reasons: appetite, relief from nausea, relief from pain, to be able to sleep.”
On the night of January 27, 1990, a squad of SFPD narcotics officers raided the house on 17th Street where Dennis was taking care of Jonathan. This is a mix of his recollections: “The police broke down my door, came storming in and found four ounces of Thai weed in the house… Jonathan was very thin and he had KS [Kaposi’s Sarcoma] lesions on his face. The cops made AIDS jokes and they made a big production of putting on their rubber gloves before tearing up the place. When they saw the picture of me and Harvey [Milk, the supervisor who had been assassinated] they went into a harangue about ‘that fag.’ They put everyone on the floor including Jonathan —they had him spread-eagled on the floor. Well, that was their undoing, because Jonathan told the district attorney and the narcs that the four ounces was his, for medicinal purposes, because he was going to chemotherapy and it helped him with his nausea and helped him in other ways. That took away their ‘marijuana-for-sale’ basis against me. They tried to link me to 27 pounds found in another house, but had no proof.”
Dennis said he recognized one of the raiders as a former bodyguard for the late Mayor George Moscone. “I told him, ‘Great job you did protecting George.’”
A vision of the cannabis buyers club came to him later that night, Dennis says, as he was lying on a cement slab at the Mission Station. “The cops were coming by and banging with their nightsticks and yelling, ‘Hey, Peron, we’re gonna get you!’ And I was thinking about Jonathan all alone and without any marijuana. And I was thinking ‘Wouldn’t it be great if there was a place where he could go and be among friends?’ Jonathan had the KS on his face and I was thinking, ‘He wouldn’t be ashamed here.’ And the place in my dream was the buyers club.”
Jonathan West died in September 1990, soon after testifying at Dennis’s hearing that the confiscated pot belonged to him. At the end he was down to 90 pounds. “Doesn’t that tell you something?” says Dennis. “He lived to testify at my trial and then he let go of life.”
After Jonathan died, Dennis shifted his approach from advocating marijuana legalization to promoting its medical use. In 1991 he drafted and organized support for the aptly named Proposition P, whereby “The People of the City and County of San Francisco recommend that the State of California and the California Medical Association restore hemp medical preparations to the list of medicines in California. Licensed physicians shall not be penalized for or restricted from prescribing hemp preparations for medical purposes to any patient.”
Prop P carried San Francisco with 80% of the vote. The Board of Supervisors then passed a medical marijuana resolution introduced by Terence Hallinan—which Dennis cited as “the authority by which the buyers club will supply cannabis and other hemp byproducts to those who can benefit by it.”
In designating his marijuana emporium at 873 Sanchez Street a “cannabis buyers club” in late 1992, Dennis was tipping his hat to the nearby Healing Alternatives buyers club, which had been established to lower the cost of vitamins, supplements and drugs rumored to slow the progression of the virus (such as AL-721, an Israeli egg-yolk extract that was commercially unavailable in the U.S. and had not been approved by the Food & Drug Administration).
Healing Alternatives was a truly non-profit organization that provided products at wholesale prices not just to HIV-positive men but to thousands of Castro district residents determined to bolster their resistance. At the SFCBC, Dennis provided discounts as needed to AIDS patients, but would not abandon the buy-low, sell-high model he had used for years as a dealer. He saw the club as part of an entourage of caregivers —Healing Alternatives providing vitamins, Project Open Hand providing food, the SFCBC providing marijuana and a comfortable setting where it could be used and shared.
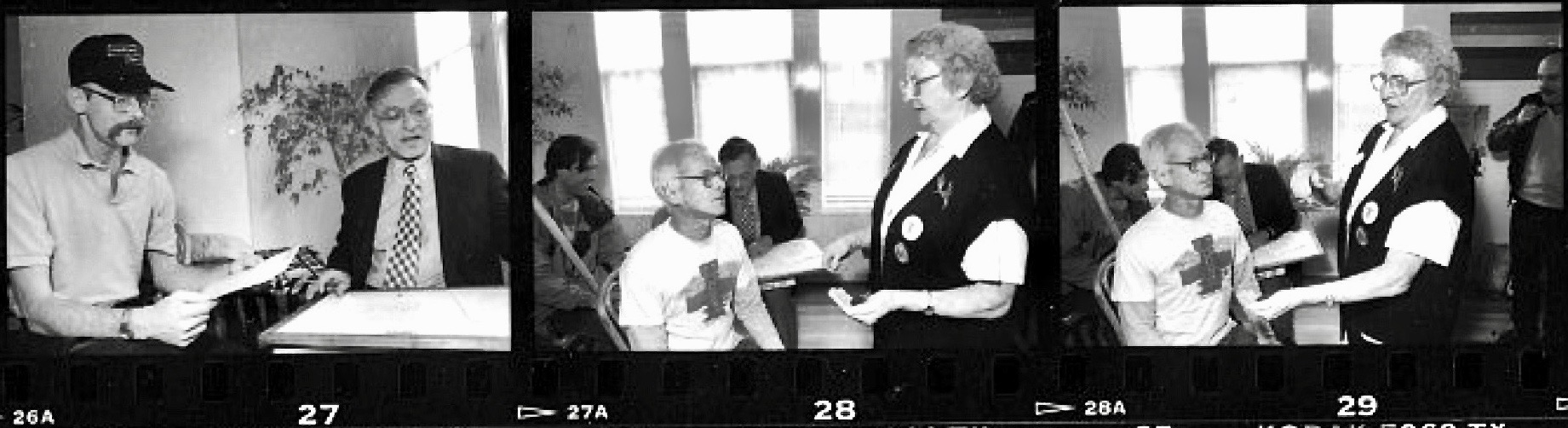
Dennis’s longtime ally, Tod Mikuriya, MD, wrote an admissions protocol for the SFCBC and interviewed members for a paper, “Cannabis Medicinal Uses at a Buyers Club” that never got published in the medical literature. The historically significant manuscript is part of the Mikuriya collection at the National Library of Medicine, and can be found online here.
While 41 of the 57 patients Mikuriya interviewed were HIV+ (and 16 “presumed HIV-“), his questionnaire documented that cannabis was being used to treat a wide range of other problems, including insomnia, depression, anxiety, panic attacks, arthritis, pain, and alcoholism. His study would provide support for the sentence in Proposition 215 authorizing physicians to approve marijuana use in treating any condition for which it provides relief.
Rick Gerharter of the Bay Area Reporter photographed Mikuriya conducting interviews —with help from Dennis and SFCBC staffer Mary Rathbun (“Brownie Mary”)— in January, 1994. The BAR ran a weekly list of people who died from AIDS — the toll was 33 one week at the height of the epidemic. The effective “cocktail” wasn’t available until 1996 (the year Californians voted to legalize marijuana for medical use).
Response to the AIDS epidemic laid the groundwork for the medical marijuana movement in other ways… (Text continues below contact sheet)
The Compound Q Saga
Today, with protease inhibitors greatly extending the lives of HIV+ people, it is hard to convey the level of fear and factual confusion (could the virus be transmitted by saliva?) that prevailed in San Francisco in the 1980s and early ’90s. See Epidemic Memories and The Party for David M.
As the death toll rose, people with AIDS —as individual citizens and in groups such as Project Inform and Act-Up— demanded with increasing urgency that the FDA accelerate research and allow access to unapproved drugs. The drug that got people’s hopes up most dramatically was “Compound Q,” a Chinese cucumber extract that researchers at SF General Hospital confirmed could kill the virus in the test tube. In May 1989 a clinical trial led by Paul Volberding, MD, was begun at SFGH. That very month, activists obtained a large quantity of Compound Q from China (where it was used to induce abortion and to treat certain types of uterine cancer). The trial they planned would not require people with AIDS to be treated with a placebo in a control group. The Compound Q saga is largely forgotten, but this being Pride Month, we’ll recount it, starting with a report published August 1989 in Synapse, the UCSF weekly. Author Kim Grahl, then a second-year medical student, is now an MD practicing in Chicago.
Meetin’ at the Buildin’
In September 1989 Project Inform organized a meeting at the Women’s Building in San Francisco to bring the community up to speed on Compound Q, the drug many were pinning their hopes on. A standing-room-only crowd —almost all young men, some visibly ill, all intensely interested— filled the large auditorium and its balcony to hear Dr. Larry Waites explain:
“Compound Q, which has been known in its present form in China for about 20 years, had been known in the US for about 2.5 years. The trials at SFGH started this summer and it was estimated that they were going to need 9 to 12 months to complete. This lengthy approval process frustrated patients and physicians. Very frequently Al and Marty and I would be together talking about early intervention and treatment. In March we realized that there were at least hundreds of doses of the drug coming into the Bay Area. We perceived an impending crisis. It was obvious that the phase 1 trial planned at SF General couldn’t possibly answer the questions about the safety and efficacy of compound Q in time to either avert or guide community use. Martin asked us if a program could be devised that was faster and yet as safe as the FDA approved trial. The dilemma was: should we wait passively for people to treat themselves. literally in their kitchens, and patch up things when they went wrong, or to take a more active stance and set up a carefully controlled monitoring situation to answer the questions about the safety and efficacy of this drug. The decision seemed obvious then and it seems obvious now that we really had to act.
“The next two months were spent in literature research, consulting Chinese physicians and even Genelabs and Mike McGrath at SFGH to write the protocol. We knew that the Chinese used 1 to 2 vials –1.2 milligrams per vial— to safely induce abortions. We knew that they used a vial per day for five days to treat cancer. We knew that in the test tube studies, cell death occurred for up to four days after the drug was given. That meant that there would be period of relative immune suppression after the drug was given –because even an infected cell may have some function and may help to fight infection. So if you kill off all those infected cells, you would have a relatively suppressed immune system. We calculated that it would take at least three doses or maybe more to possibly kill all the infected tcells and macrophages. Thus we decided to treat people once a week for three doses, to start at 1.2 milligrams –17 micrograms per kil0. We decided on very intensive monitoring of patients.
“Our first three patients were our very sickest patients. they’d exhausted all other avenues of treatment. We saw them just about every day. The protocol called for following patients overnight after they got the infusion, seeing patients the day after the infusion, then each week of the first month, then monthly thereafter. We had very extensive lab work consisting of complete blood counts, panels to check liver and kidney function, urnialyses, blood work done weekly, then monthly, as well as checking p24 antigens and antibodies. Cost of lab work alone for first 6 weeks was over $42,000.
“Was this all legal? Our lawyers said yes. We now have 7 lawyers. The FDA does not interfere in the right of patients to obtain medicines from any country for their personal use, nor does it interfere in the doctor patient relationship. Our treatment program differed only in its intensity of monitoring and the lengthy informed consent process, which started three days before the infusion.”
Compound Q failed. The unauthorized trial showed that the cucumber extract did not, alas, fend off the AIDS virus in the body. But the episode focused the gay community critically on the FDA drug approval process, and reminded us, the people —and our rulers— that drug prohibition could not be enforced on those who felt they had nothing to lose. By the start of the 1990s, increasingly large demonstrations and street actions* signaled that the demand for AIDS support services (the virus had pushed thousands into poverty) and research leading to effective treatment had become a mass movement.
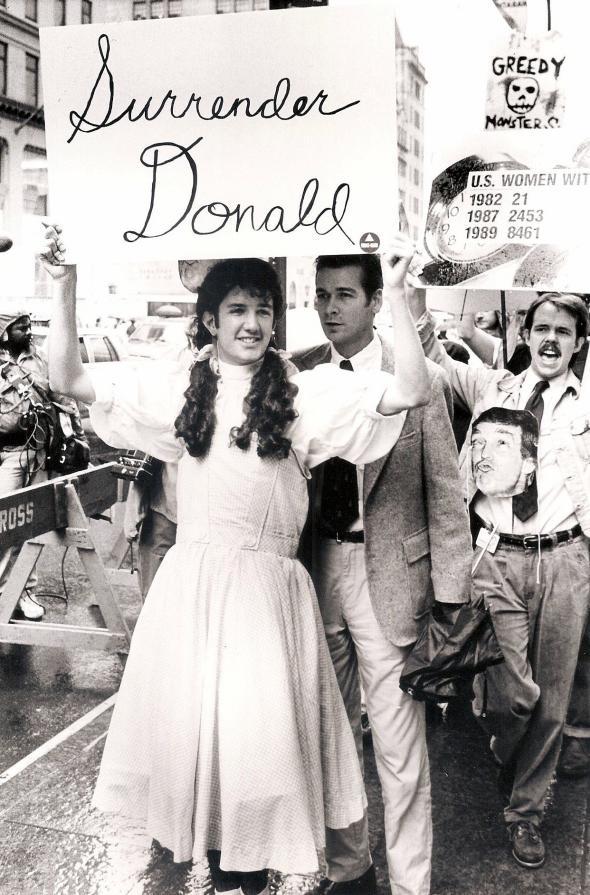
- Including a march on Trump Tower in New York, staged by ACT-UP on Halloween, 1989. “The Trump Tower protest was organized by ACT UP’s Housing Committee, which hoped to draw attention to the lack of housing for homeless people with AIDS,” wrote Stephen Vider in Slate. “Through the rain, protesters maintained a picket line, carrying a range of printed and handmade signs: ‘Silence Equals Death,’ ‘In NYC 10,000 Homeless PWAs, 64 Beds,’ ‘Money For AIDS Not For Malls.’ Two participants hung a banner, ‘10,000 Homeless With AIDS,’ from the windows across the street.”
A Not-so-Proud Memory
It’s Pride month, but we owe it to history to recall an embarrassing, tragic twist in the relationship between AIDS activism and the medical marijuana movement. By 1998, ACT-UP San Francisco was being led by a small group of men who refused to acknowledge that AIDS was caused by the Human Immunodeficiency Virus. They were desperate, militant, and not interested in treatment because they thought the virus wasn’t causing the epidemic. They cited a UC Berkeley molecular biologist, Professor Peter Duesberg, who contended that people were being killed by use of recreational drugs and AZT, an early FDA-approved treatment that turned out to be ineffective.
Several leaders of ACT-UP San Francisco worked at Dennis Peron’s cannabis buyers club, and when the state and federal governments finally succeeded in closing him down in 1998 —as a nuisance!— these staffers knew how to run the operation and knew all the growers. They launched a club of their own further up Market Street —more a sales outlet than a place to socialize— and were soon bringing in $100,000/month. The money from marijuana sales at the ACT-UP club was used to fund a big denialist PR campaign. Denialist literature packets were dispatched to government agencies worldwide, and Thabo Mbeki, the president of South Africa, took the ACT-UP/Duesberg line seriously. The distribution of effective protease inhibitors in his country was delayed as a result.
The moral of the story is relevant to pot partisans today: Don’t totally turn your back on Western Medicine!
That said, the list of FDA-approved drugs that have turned out to be ineffective and/or harmful is mind-blowing. An O’Shaughnessy’s article about FDA reversals will run when we can pay the printer again. The AIDS denialists were crazed, for sure, but the abysmal record of the pharmaceutical industry gave their worst paranoid suspicions a germ of plausibility.
PS June 28
No sooner did I write the above than the July Scientific Americanarrived with a letter by Dr. John P. Moore on the subject of AIDS denialists. Moore attributes an estimated 300,000 deaths worldwide to their influence. Asked for his source, he explained in an email, “There were two articles published in the peer-reviewed literature sometime around 2005. One was from a group at Harvard Medical School and received fairly wide publicity at the time, the other was from Nicoli Nattrass of the U of Cape Town. Both were quite concordant in their estimates, which were made independently.”
“The AIDS denialists are still around,” according to Moore. “Their damaging effects have diminished in recent years, but many of them are now active in the ‘anti-vaxxer’ movement, peddling the lies that compromise vaccine uptake by a significant number of people, with adverse public health outcomes that are all too apparent.”
I asked Moore, “Was almost all the impact in South Africa? It seemed like the denialists made a lot of noise but didn’t deter people from going on the protease inhibitors when they became available in ’96.”
He replied: “it’s a highly complex and lengthy topic that can’t easily be summarized on an iPhone email from home. In the developed world the denialists did not affect national policies but did damage individuals who were persuaded to make very poor choices about their health or their children’s health. But in South Africa in the early 2000s the Mbeki administration was persuaded to take some catastrophic policy decisions on drug availability that led to those estimated 300,000 unnecessary deaths. Books on the topic include ones from Nicoli Nattrass, Seth Kalichman, Jon Kay and Michael Specter if a longer version appeals to your reading list.”
An Interview With Martin Delaney
By Fred Gardner for the Anderson Valley Advertiser, September, 1989 Martin Delaney is the prime mover behind the community-based trials of Compound Q recently conducted by private physicians in San Francisco and several other cities. The trials challenge the authority of the United States government, the medical research establishment and the pharmaceutical industry. Delaney’s audacity comes from his constituents —AIDS patients who feel they have nothing to lose. His charisma, his intelligence and his ability to formulate a plan and carry it out come from God knows where.
Delaney was born in Chicago in 1945. He grew up there, went to Catholic schools, one of five kids. His father was a machinist, his mother a housewife. He dropped out of a seminary in the late ’60s, became a teacher and then a negotiator for both teachers and school systems. He developed a business in which he taught negotiation skills. Stricken with chronic acute hepatitis and assuming he had only a short time to live, Delaney moved to Sausalito at the end of the ’70s. He got into a treatment program at Stanford that saved his life but was subsequently abandoned —leaving him highly critical of the way drug research is controlled by bureaucrats.
In the mid-80s he founded “Project Inform” to help AIDS patients gain access to experimental treatments. Project Inform has long advocated that people who may be at risk for AIDS get tested (a position that incurred the wrath of many “civil libertarians”), and that people who do test positive should start taking AZT before they show symptoms. Both these positions have been validated now that AZT has been proven to slow the progression of HIV infection.
When I interviewed Delaney at his Sausalito apartment on the last day of August, he was tired. He had just gotten back from several days in Washington, D.C., where the government is about to issue new guidelines legitimizing the “parallel track” approach to studying new drugs.
As we spoke, the doctors who conducted the San Francisco study of Compound Q were preparing to submit their preliminary data to the Food & Drug Administration. They will characterize the drug as “promising.” Q, it will be reported, has a measurable antiviral effect on AIDS patients. It appears that Q, unlike AZT (which prevents the virus from replicating and infecting new cells) actually lowers the reservoir of infected cells in the body. In other words, it appears possible that Q will have a role to play, possibly in combination with AZT, DDI and other drugs that slow the course of the disease
But Q, the doctors found, can also have dangerous side effects: it can induce dementia and coma in people with large numbers of HIV-infected brain cells. This may occur because as Q kills the infected cells, substances are released that interfere with the function of surrounding tissue in the brain. Fortunately, it appears that the comas may be avoidable (they have all been preceded by dementia) and both symptoms are reversible (by administration of a steroid called Decadron).
AVA: How did Project Inform get off the ground?
MD: It evolved in that period, 1984-85, when nothing was availble to treat the disease. A few compounds had been identified as having possible value. One was being widely used in the community because of its availability in Mexico. Project Inform was founded initially to collect research data on that phenomenon, to answer the question was this a good idea, a bad idea, a waste of money? We didn’t succeed in raising money to do the research at the time. It was sort of outside of our turf and a lot of people were offended –the doctors were offended by our being on their turf. So our emphasis shifted. If we couldn’t get the research, at least we could get the best possible information on this stuff. What doses were were appropriate? What were the side effect dangers? How could they be minimized? So we shifted into being more of an educational institution than providing data, first on that, then on everything else that came along as treatments for AIDS.
AVA: I understand you’d had a run-in with the medical establishment before this.
MD: In the late ’70s I had chronic acute hepatitis. [About 10% of people with hepatitis don’t throw off the virus and develop chronic hepatitis. About10% among remain in a repeating cycle of acute hepatitis which eventually kills them.] I moved out here knowing that. I was disabled, very weak, very thin, looking like a little old man. Didn’t digest food properly. All the end-stage hepatitis stuff was going on. Eventually I got into a clinical program at Stanford, and in the course of the treatments I came back to life. I could clearly tell that a huge difference had taken place around the fifth month of treatment. Suddenly my energy came back, my weight came back, it was like a switch had been thrown that had been shut off.
AVA: That’s great!
MD: Yeah it was, it was exciting. The problem was I still had a month to go in the therapy, and I continued, and near the end of the sixth month I suffered a side-effect: neuropathy. It’s never healed, but I’ve never had any regrets over it. To me it was a perfectly fair trade off, and I would of course do it over again, even fully knowing about the neuropathy. And the neuropathy was as bad as neuropathy gets –a terrible burn. But it was preferable to an early death. It appeared first in my feet. There’s no way to describe it except as an absolute burning sensation around the bottom of the feet, and over the next months it spread upward toward my knee. Up in the leg it wasn’t burning, it was muscle weakness, muscle pain, loss of sensation. I eventually lost the muscle control over my toes. For the most part it could only be treated with pain killers, and over the years it has changed some. It doesn’t burn now, it’s more like an electrical sensation, but it’s still controlled with painkilling drugs, and that’s a bit of a nuisance, but still I don’t regret the choice… I still to this day go down to Stanford every 30 days and get a supply of methadone. Methadone is an excellent pain killer. It doesn’t slur your speech or make you dizzy. Within three days of starting it I was ready to go back to work. It’s a drug with a lot of negative connotations because of the association with heroin and because it’s considered a Nazi drug (laughs).
AVA: How did the idea for the trial of Compound Q get formulated?
MD: A big factor to me was realizing that the community had already found a way to import it. People down in Florida and one other city had already found a way to get the drug as early as last February (89). The stories were circulating in the underground networks, so already people were doing it. The earliest people who got it did so by contacting hospitals over there, they made relationships with individuals in hospitals who in turn sent a box here, a box there as a compassionate action –they weren’t even charging for it. That in turn led to other “couriers” starting to make trips over there and feeling things out. I talked to one who had been one of the leading couriers in getting some of the other drugs, and he was sympathetic to the notion that we should do it differently this time. He agreed with me that we should do something different this time and it shouldn’t be turned into a market. Especially because as a a chemotherapeutic agent, this was going to be a dangerous one. This was not herbal tea. A lot of the community wanted to see it that way, of course: because it was Chinese, it was associated with cucumbers, it was organic… So all of that we saw as a formula for disaster. A single shipment could provide the drug for thousands of people. And usually the first ones to do this are the most desperate people, people on their deathbeds. I think we would have seen hundreds of deaths occur, and that prospect is still out there if there’s unprincipled use of the product. So our point was to head that off, to make sure that this individual courier didn’t turn it into a business –fortunately he went along with the notion– and in a sense, fulfill the old original mission of Project Inform: collecting prospective data on a treatment protocol
AVA: How did you find the doctors?
MD: We knew not many doctors were going to be willing to stick their necks out on this one. It was an injectable substance, they quickly would see the risks involved. Also, we needed doctors who were serious about data collection. Unfortunately, most GPs treating AIDS are not. They have really no idea whether AZT is helping or hurting their patients. They have anecdotal feelings about it, but they don’t collect data. So that led to turning to Al Levin and his associates, one of whom is the researcher behind Risin-A, another ribosome inhibitor protein, probably the closest thing to tricosanthin that had ever been developed in the US. She works with Xoma corporation and manages their clinical programs. She has designed and carried out studies on about 1,000 cancer patients using that drug. So she was a natural, as was Al.
AVA: Tell me about Al
MD: Al’s a controversial guy, but if you look historically, most of the things he’s been controversial over he’s been right over. Two years ago he was attacked by the medical establishment because he had opened up a clinic and claimed it made sense to treat people in early intervention, claimed that low-dose AZT made sense and that doctors were overmedicating… He was accused of quackery and everything else for that –but now, two years later, it has become medical orthodoxy, proven facts. One of the ways he had reached those conclusions earlier is that he runs an elaborate 40-point data base on about six or 700 patients that they follow on every possible paramater. That kind of serious record keeping was very attractive to me. It’s frankly what the whole system should have been doing all along. Every patient with AIDS should have been in such a data base. We’d have known much more quickly about the effects of AZT and the side effects of various drugs and underground treatments and everything else. Dr. Abrams is now doing that, too, with the county consortium’s registry project, which was forced down his throat by the community but now he acts like it’s his idea. So anyway, Levin had the data base and he was willing to do it. He also had a sophisticated clinic facility. I began feeding him information from the Florida group. It was probably in April or early May that we began talking about doing a treatment protocol, and that led to beginning with the first patients at the very end of May. There was no recruiting necessary. There were many people who had expressed a strong interest in getting Q if they could –it was all over the newspapers– and who met the definitions of the protocol, which were the same as SF General’s, which is where we lifted them. The window of patient health: more than 1,000 white count, T cells under 400, evidence of positive p24, all those measures that made it possible to measure the outcome. All but one patient in our study actually had T cell counts below 100. I think that was appropriate because there’s a general rule in phase 1 testing is: you go first with your sickest people, with whom you have the least to lose, so you’re not risking years of someone’s life if soemthing goes wrong. So the very first patients, God, I don’t think the first 10 had 50 T cells between them.
AVA: So Levin is now collating his data…
MD: I don’t think the data is as well put together as we’d like it to be. Al is by nature an optimist. Genelabs and Sandoz [The Swiss-based multinational that bought the distribution rights to Compound Q] have opened up an account for us at an independent firm called Fairfax that does analyses of other studies. The data will be turned over to that company for a formal statistical analysis. We will probably have our own analysis completed before that. I think it would be a mistake to draw any conclusions before we’ve analyzed all the data. There have been certain indicators all along that have worked the way we wanted to see them work, in particular the p24 numbers, the main measure of viral activity, I’d be very surprised if the data suggested that was a coincidence. All of that has to be balanced against the fact that the drug has the potential for some serious side effects, at least in the sickest patients.
AVA: What is the doctors’ hypothesis –why do side effects occur in late-stage patients?
MD: There are two hypotheses involved: one is that there’s a factor released by infected macrophages that is responsible for AIDS dementia in general, and that the drug may be causing some release of this in patients who are already putting out that factor. The other idea is that it’s the result of killing infected cells in the brain, resulting in some degree of temporary disruption. I think it’s clear from evidence we’ve seen that when this occurs, it’s a manageable problem. It’s manageable with the use of Decadron.
AVA: Does the Chinese version of the drug differ from the Genelabs version?
MD: There doesn’t seem to be a substantive difference. For a while Genelabs and SF General were implying that the problems we saw with patients should be attributed to some impurity to our version of the drug, or some fuck-up on our part, and now they’ve had to acknowledge that that’s not the case, that it’s an inherent quality of the drug in certain patients, and we think it’s tied to a therapeutic action of the drug that perhaps has a harmful consequence if it isn’t managed properly. But it points to the fact that the drug is killing the infected cells. And we’re not going to abandon this drug if it does that.
AVA: What happens next? What’s the Compound Q scenario?
MD: All the doctors involved in the study will meet with the FDA in Washington. to lay out our preliminary assessment of the data. We’ll talk with them about the possibility of setting up community-based trials. I have a feeling that that notion may be discouraged now because of SF General’s problem with their comatose problem. Both the drug company Genelabs and the FDA are going to push for more carefully controlled clinical settings. I understand they may be taking it out of SF General and putting it into the hands of Stanford. AVA: McGrath couldn’t run the study, I gather, because he’s not a clinician and he’s the developer of the drug, has a financial interest in it. MD: Yes. And I think McGrath was told to stay away because he was passionately concerned. He was questioned as to whether he’d had any contact with us.
AVA: How would you characterize your relations with Paul Volberding? [The doctor at SF General running the FDA-sanctioned clinical trials]
MD: I’ve met with him over many issues that concern the patient community –protocol design, research practices and policies. Sometimes we’re adversaries, sometimes we’re collaborators. The issues I deal with are not medical issues, they’re much more the philosophical and psychological issues. And in those disciplines I have more training than Don Abrams and Paul Volberding put together. I’m not arguing medicine with them, I’m arguing philosophy over patient rights, the level of risk versus benefit, those are ethical issues. I also would argue that when it comes to medical issues and AIDS, everybody started learning those at the same time. Don Abrams did not learn about AIDS in medical school, and neither did Paul Volberding.
AVA: I understand that a doctor named Shelley Gordon had written in a patient’s chart that his symptoms were attributable to “impurities” in the Compound Q he was receiving from Levin. You were informed of this entry and wrote a letter to the hospital protesting the reference to impurities. And Gordon then expressed outrage that Martin Delaney was reading her patient’s chart.
MD: That kind of arrogance is exactly what we’ve been trying to drive out of the medical community. That kind of God-like power: the doctor is in charge, the doctor runs all this, nobody has any right to discuss it or think about it. Gordon was totally out of step with the changes that have been taking place around AIDS, which is a much more collaborative relationship between patient and physician. She made a powerful case for why things need to be different.
AVA: What’s your political history?
MD: I don’t think of myself as having much of a political history. If anything I was conservative in my seminary days. I went to St. Mary of the Lake in Mundiline, Illinois. It’s considered the West Point of the Catholic Church. I was the middle kid of five kids. My dad was active in the Democratic party. Our family had a connection to the Daleys. I had an uncle who was a priest who was the pastor of the mayor’s parish, so all through my childhood we had this link to what was going on with the Daleys. If something was going on in their parish, we would be part of it. We knew each other –not on a close social basis.
The Democratic Convention did radicalize me somewhat. This was shortly after I had left the seminary. I was simply going down there out of curiousity. This was my town, Chicago, so I went down to Grant Park. I didn’t see crazed hippies in the streets. I saw middle America protesting the war –with an occasional crazed hippy somewhere with all the cameras centered around him. But there were thousands and thousands of ordinary people who were part of the movement to end the war, and I was certainly sympathetic to that. By sheer coincidence, I got arrested. I was down there with a couple of friends, some of whom were still in the seminary, some of whom had left at the time I did. We had gotten separated. This was Wednesday, which turned out to be the cataclysmic night. We had gotten separated in the crowd because of tear gas.
I was being radicalized by what I saw, because I truly did see what the Walker report called a “police riot.” The police were just crazed in Chicago at the time. Beating people relentlessly, mercilessly. I saw them beat pregnant women, tossing people over railings, into subway stairways, stuff that I was just aghast at seeing. I had never seen anything like it in my life. It was an incredible event. There was an intoxication of it, too. Thousands of people, police on horses, the world media covering it. Anyway, we got separated –I had to take somebody back to a car, and then there was the tear gas– and we had pre-arranged to meet with the rest of the group at the corner of Michigan and Balboa, outside the Conrad Hilton, not knowing that was where everything was about to happen. So at 10 o’clock I came back, kind of struggling my way through the crowd to catch up with the folks, and that was where everything was exploding and everybody in sight was being shuffled into police vans.
I got shuffled into a van with a nuclear scientist from Sweden named Leif Erickson who was staying in the Conrad Hilton. He was trying to get back to his hotel. There were 17 of us in this van and we were all thrown into a cell. We were all mystified: ‘what have we done? why are we here?’ We were ultimately sat down with a good Irish Catholic desk clerk at the office who made up a story about our arrest. He told me what he was writing down, making it up as he went along. I said this is nonsense. Each van was assigned to a sergeant’s name. Our van was assigned to a Sergeant Rojack, who of course hadn’t arrested us, and they sat there and made up false arrest reports right in front of us.
I said to the desk clerk: “How can you possibly do this and still go to chuch on Sunday?” And he says: “What were you doing down here in the first place? Don’t give me any belly-aching. You didn’t belong here so don’t complain about what we’re doing.” Later it became very clear how each group was being handled, we were literally being asked for a payoff, that’s how things worked in Chicago. There was a strict figure set: 600 bucks, that was the cost of getting this thing taken care of. My family was just aghast. We couldn’t believe that this was our city, that this was our mayor. My mother called the Mayor on it, I sat there and watched while she called the Mayor, and they got into a sputtering screaming fight where she finally slammed the phone down and that was the last time we ever had any contact with the Daleys.
He had used a line on TV when they were questioning him about it all, “What trees do they plant?” This was his line in about the protesters, implying that they don’t accomplish anything, and he repeated that idiot remark to my mother –that was what caused her to hang up the phone. She said “‘What trees do they plant?! You moron!” and slammed the phone down and that was the end of that.
So in the end it came down to having to pay $600– that was the way it was done. We finally got the money together, brought it down there and we gave it to the attorney and right in front of you he handed off x amount to Sgt. Rojack. That’s the only time I ever saw Sgt. Rojack, when he was getting his payoff. $25 went to the city clerk, $75 to the judge and I’m looking at this and I can’t believe this is going on. Finally, I said “And you expect me not to say something about this?” And they said “look kid, you gave us the money, so if this is bribery you’re a party to it, you started it so you’d better keep your mouth shut.”
And it’s true. I called Mike Royko that day and he said, “I got this story from several hundred people and I can’t print it, because I can’t verify it. Nobody other than individual citizens like me will go on record that this has happened.” I said “why can’t you just take our word for it?” He says “I know it’s happening, but I tell you I can’t print it. You don’t understand how Chicago works. I can’t print this story.”
AVA: From ’68 to the present –how did your perspective develop?
MD: There wasn’t much politics from ’68 up to the present. I didn’t do much and there wasn’t much happening politically. People withdrew, we got mediocre morons to run the country, nothing has been happening since, so I’ve had nothing to do with it since. I I was burned enough by the Democratic convention and discouraged enough that I just wanted nothing to do with it. I just wanted to get on with my life. The hell with it, they were just all liars. The Democrats I’d believed in turned out to be crooked liars just like the Republicans, and the Republicans were the elitist morons that everyone said they were, so I had no taste for politics. The only other thing I’ve ever done in the politics was in the late ’70s before I moved out here, I had begun providing skill training for leaders in the gay movement in Chicago. I developed a friend in that area, and it was so clear that they didn’t have even the most basic business skills of communications and interactions and how to work with people, and this was stuff that I taught in my business and wrote on.
AVA: Tell me about your business and how you make a living.
MD: Right now I’m with Project Inform, but before that I was a consultant developing educational programs in a corporate setting. I write seminars, I deliver seminars, I write and produce educational videos, instructional videos in a corporate setting usually dealing with one of three subjects: negotiations; sales and marketing; and quality assurance. I do that primarily in high-tech industries and in financial services, banks and brokerages. I’m a private consultant in instructional design services.
AVA: How did you get into that field?
MD: By hook, by crook. Originally I had taught in the public school system –fifth grade. Then I moved into an administrative position within the school.
AVA: In the Chicago public schools?
MD: No, the wealthy suburbs outside Chicago. I was probably more vibrant than your average teacher, and they wanted to make more use of me. So I was working in administrative functions setting up resource centers, groups from various classes. I did that for about six years and while doing that I also got trained as a union negotiator to negotiate teacher union contracts for the unions. In the course of doing it I realized that it was a skill and I could do it either way so I hired out on the other side of the city doing it on behalf of school districts. As long as I stayed out of my own turf it didn’t matter, so I took that on as moonlight work. I think I learned a great deal about negotiating in that process because we were trained to negotiate in traditional ways and I quickly found that all the traditional beliefs about negotiation actually interfered with the ability to get an agreement. Your traditional training taught you how to posture and drum up your troops and pressure tactics and manipulations and all that, but in the end, every time you made an agreement, it only came after you had put all that bullshit aside, and you finally quietly sat down with another human being and made a fair agreement.
That had a profound impact on me, that realization that all that other stuff we believed as a culture about negotiation, the machoness of it all was what made it a problem, it wasn’t the solution it was the problem itself. That later on became something that I taught as a businessman. I turned that into a philosophy, a program about negotiation and I’m hardly the only one to have had that insight. The Harvard Negotiations Project does the same thing. But that started in one way to lead me into things that I do now. Eventually I reached a pointed where I just got tired of it all, having to please the Boards of Education, the Teachers’ Union, the kids, the parents. Do i really need all this for $12,000 a year or whatever it is that teachers got paid back then?
I just resigned and I didn’t know what I was going to do, but I’ve always had this sense of luck or good fortune in may life that something would happen and I left at the end of that school term and sure enough there was a corporation out there that needed somebody who could do standup instruction. I began working with a division of the Xerox Corp. originally as an independent contractor, giving seminars that they had written. I did that for a couple of years and later became an employee of the company and sold for them for a while. I began doing some design work for them. My frustration in that was working in a corporate setting, had to work in these little niches where you only did this and I had something to say about every aspect of the corporation. I wanted involvement in how the product was designed and sold, how the company was managed etc. so I realized that I didn’t fit into corporate America, at least not a big corporation, I wasn’t one to sit in a niche and keep his mouth shut.
I broke off from Xerox and worked for a few years for a small company in the same field. That was all right but it was too personal, your personal life got all wrapped up in the personal lives of the other people in the small corporation. That wasn’t for me either, so I just broke off and began working on my own and have been doing that ever since.
AVA: When did you get sick?
MD: I first knew I was sick in ’76 or ’77. I knew I’d had a mild something, I didn’t know what it was. It slowed me down for a while and then I noted that it came back and seemed to be recurring, still didn’t know what it was and I was never serious enough to pay any attention to it. A friend at one point had gotten hepatitis and had urged his friends to go get checked in case he might have spread it. So I did, and sure enough the tests showed that I did have hepatitis and that sort of led to an explanation of what was happening to me. Originally it was recurring every six months, then three, then two. Each time it would recur it got worse and I would get weaker and weaker, and the blood work indicated that this was hepatatis again. My doctors finally got alarmed by it and said, “look, this is not normal hepatitis, it looks like chronic hepatitis and more than that it looks like chronic active hepatitis, and you’re going to have to do something about it very soon because this is the profile that people die from.” So I just got very scared and I moved out of Chicago. That’s one of the reasons I came here. It partly was the sense that if I wasn’t going to live, this is where I wanted to spend my final years. I loved it out here, I used to come out here and visit every summer. Also, there was a group out here that I wanted to contact, the Center for Attitudinal Healing in Tiburon, that deals with people in life- threatening situations. In the end I never did contact them because I decided to live instead. I moved out here, to this apartment, as a form of convalescence.
AVA: How did you find the Stanford study?
MD: I was sitting in this very seat one day, and a friend walked in the door waving a newspaper and there was a little paragraph in there where someone named Merrigan at Stanford had a program and was looking for patients with chronic active hepaptitis to do research . I went out there and it took almost a year before I got in it, but finally did.
AVA: is it true that the program was abandoned?
MD: Yeah, it was eventually was shut down. There was a feeling on the part of the researchers, actually more the government, that the risk versus benefit wasn’t appropriate.
AVA: The risk was neuropathy?
MD: It was as serious a form of neuropathy as you ever get; a lot of drugs have been shut down because of neuropathy. AVA: But why in a life-threatening situation would anyone think pain…
MD: Neuropathy is a reason to shut off a treatment for a life-threatening situation? You tell me. You got me. That was the frustration, because over the years I saw friends die from hepatitis who didn’t have the chance to try what I had. Now that’s not to say that it would have worked in every case, but it did work for some of us, I was not the only one who had a profound change of condition as a result of the treatment.
AVA: So that was your real first exposure to the world of biomedical research…
MD: Yeah. And it taught me that there’s something wrong when people with life-threatening illnesses are having the shots called for them by bureaucrats in Washington. It didn’t make sense to me that a bureaucrat in Washington should decided whether someone with chronic hepatitis had a right to try this treatment or not. If your life is on the line, you and your doctor should decide what to do about, not some bureaucrat in Washington who doesn’t know or particularly care. When AIDS came along, I really knew there was something profoundly wrong with the way the medical system looked at people with life-threatening illnesses. But at first my attitude was sort a “so what? it isn’t going to change my life.” But it did when friends and people close to me started falling from AIDS. Those issues became very stark right away, here we were in that situation again. People were dying, there was no hope being offered, and the government was saying ‘you can’t try this, that or the other thing which we have but you can’t because we haven’t decided it’s safe for you yet.’
AVA: How big is the staff of Project Inform?
MD: There are five full-time people and about 70 volunteers. At any given moment there are 12 people on duty at the office. There are always five on the hot line while the others are spread around doing various things like mailings and related tasks. This year the budget will reach close to one million dollars, but it keeps growing so fast that I can’t tell you what it will be next year. We don’t have the luxury to operate the way a long-term foundation does. We view this as an emergency operation, not a piece of turf foundation-wise. Our goal is to shut it down, dismantle it, so we are very disinclined towards lots of staff with layers of management. Most of the money that comes in to us gets turned right back into services. Sometimes we’re criticized for that by other foundation groups –they feel uncomfortable with our”lack of organizational infrastructure.” I’m uncomfortable with their excessive organizational infrastructure. I think AIDS organizations ought to view themselves as emergency ad hoc functions, not as opportunities to build organizational turf.
AVA: What really drives you, Marty?
MD: Every day I get calls from people all around the world who are dyng. And no matter how much success we feel we are achieving in Washington, it’s never good enough. It’s never fast enough, it isn’t remotely good enough to meet the need that’s out there. We are about to celebrate this great victory, the creation of parallel track drug testing, early access to experimental treatments. People think this is just a momentous event and a huge shift of power. Tell that to the 40 guys who called me yesterday who couldn’t get DDI next week and may die because they are past the point of no return. I’m just haunted by that. Last Sunday I went to a party with friends of mine. Just before leaving a friend called who’s been sick for six years, not with AIDS but with ARC. He and has successfully combatted it for a long time, but he couldn’t come because two of his best friends who’ve had AIDS for more than two years were feeling very lonely and wanted company for dinner and could I come?
Well I couldn’t come because I was committed to this other party and I was giving blackmarket AZT to some people because there are some people who don’t want AZT on their insurance records. So I go to the party, and these are people that I’ve known for 10 years. It turns out that one of them who has been quite sick himself couldn’t be part of the party because a close friend in Chicago had died. Two others had had a lover die within the last year. The house we were in is haunted by the spectre of a friend who died a year ago, his pictures are all over the place.
Two others at dinner had to sneak out to my car so I could give them the AZT without the rest of them knowing that they were sick. In the course of the dinner I got a call from a friend in St Louis who had come down sick from the AZT which he had just started using. It just struck me as the party was ending, all but two people at the party were sick currently and even those two had lost people last year. It struck me: what kind of life is this? This is what life is like in the gay community in San Francisco? These were not people who I had met because of AIDS work, rather people who don’t even want to acknowledge my AIDS work. But this is part of their life. And it’s just like that all around us, it is a holocast. That’s what drives me.
AVA: Why does AZT cost $8,000 a year?
MD: Because Bourroughs-Wellcome sees it as an opportunity to line their coffers. Whatever the true cost of production is, it isn’t even remotely close to what it is being sold for. This was a major opportunity that the pharmaceutical companies seldom get. You have a true product monopoly with a captive audience and they’ve got it and they’ve exploited it. They would rationalize that they had to amortize their costs quickly over three years. Well, shit, the drug’s gonna be there another three years, no sweat. The American taxpayers are paying three times for that drug: we’ve paid for its initial development; we’ve paid for the studies to test it; and now we’re paying to buy it back from them. There’s something criminally wrong with a system that permits that.
Meanwhile, Back East…
The above is a Frisco-centric history of a movement that had another major locus in Washington, DC, and then Florida, where Robert and Alice O’Leary Randall helped patients get FDA approval to use marijuana on grounds of “medical necessity.” MORE TK.