By Decca Aitkenhead in the Guardian March 12. Applicable in many ways to US doctors.
‘The psychological wellbeing of the medical workforce is being completely ignored,’ says occupational psychologist Caroline Elton. All of us become patients, sooner or later, and there is no shortage of literature about our experience of the medical profession. Our health problems have produced numerous bestsellers, many of them written by the doctors who treat us. But until now I had read little –and must confess, thought even less– about who is taking care of them.
Doctors are more prone to mental health problems, it turns out, than any other profession. Their working conditions are more stressful and punishing than anything the rest of us have to deal with in a day at the office. When a junior doctor walked into the sea and drowned in 2016, her parents wrote: “Long hours, work-related anxiety and despair at her future in medicine were definite contributors to this awful and final decision.” Only last month, a trainee paediatrician killed herself following a panic attack at work.
A report in the British Medical Journal in 2011 found that a third of doctors have a mental health disorder. A Royal College of Physicians’ survey of junior doctors last year found that 70% worked on a rota that was permanently under-staffed, 80% felt their work put them under excessive stress, and a quarter felt it had a serious impact on their mental health. Caroline Elton is an occupational psychologist who has worked with medics for more than 20 years. We meet at her north London home, where she now runs a private practice offering career coaching and psychotherapeutic support to doctors. Her manner is self-effacing and unassuming, but she is uniquely qualified to comment, having been employed by the NHS for the first 10 years of her career to observe hospital consultants in action, as part of a project to make them more effective teachers. She shadowed anaesthetists, went on ward rounds, observed surgery and sat in on supervision sessions, in order to give consultants feedback on how to improve their teaching work. “So I saw what it was like to be doing a lot of these different specialties. And it was a rich induction that proved to be completely fortuitous,” Elton smiles, because she then spent the next 10 years running an NHS careers advisory service for trainee doctors across London.
She’d expected the job to be all about guiding clients towards career paths they hadn’t previously considered, but much bigger emotional themes kept cropping up. “Coping with the transition from medical school; questioning whether they were suited to the practice of medicine; the impact of exposure to patient suffering; the seeming impossibility of reconciling family and professional demands; the emotional complexity of leaving or abandoning a medical career.” The combination of careers advice and psychological counselling was “a bizarre hybrid of a job”, and one very few people are employed by the NHS to do – but she wishes there were more. “The psychological wellbeing of the medical workforce is being completely ignored.”
The technological and medical advances in medicine are breathtaking, Elton acknowledges. But this has not been matched by understanding about the psychological load doctors bear. “We’re absolutely in the dark ages,” she says.
Elton has now written a book about her work, Also Human, which introduces us to a cast of medics in varying states of despair. There is a trainee paediatrician so paralysed by fear of a baby or mother dying in his care that he kept failing his final exam, and eventually abandoned his idea of a career in medicine. Another trainee vomited at work every day from anxiety and panic. I’d be surprised if anyone who reads it will ever look at doctors in the same light again.
For many doctors, the difficulties begin as soon as they leave medical school. Final exam results determine which graduates get first choice of the available jobs across the country, meaning the weakest are most at risk of finding themselves struggling in posts that stronger students avoided, isolated, far from home in unfamiliar towns where they have no support network.
I’d assumed the European working time directive, limiting junior doctors’ hours, had broadly solved the problem of unmanageable workloads. But the problem, Elton explains, is more “like a Rubik’s Cube”, because the reduction in hours has increased the frequency of handovers, destabilising teams and leaving juniors unsupported.
Often it’s that human-to-human encounter that eases the pressure. If you detach yourself, you’re not going to get that. “I’m not saying we should go back to the old days when junior doctors were working some zillion hours. But what it does mean is you’re now working with an ever-revolving team, with different people being on different schedules and different rotas. If a junior doctor is feeling very unsure of themselves or worried, and the person a couple of steps up the ladder doesn’t know them, they may not see that this person’s normally quite chatty but is very subdued. They haven’t got that intimate knowledge of the team to pick up on it. And nobody thought this through.”
Elton’s panicked young clients report shocking indifference from senior colleagues. When one was reduced to tears by a senior and went to her supervising consultant for help, his response was: “Of course this is how you feel. You’re an F1 [the most junior rank]. You’re a girl. You’re going to be upset.” A system engineered to suppress rather than promote empathy has grave consequences, Elton warns, for all involved.
Ever since the 60s, she explains, the model of “detached concern” towards patients has been the gold standard of the medical profession. “Of course doctors and nurses have to have the capacity to detach in the moment, or in the course of an operation for a longer period of time. But we need to interrogate whether that is the correct stance for all interactions.” Studies consistently find that as their training progresses, medical students’ empathy levels steadily decline. “It should be a switch that doctors can switch on and off, but it’s seen more as a personal quality that you take into all your dealings with patients. Unfortunately, I think the switch rusts.”
Conventional wisdom has it that medics cauterise their emotions to protect themselves, but the evidence suggests that in fact suppressing their feelings makes them burn out more quickly. Elton cites a recent study that found the most empathetic doctors reporting the lowest rates of stress and burnout. It sounds counter-intuitive, but she explains: “Very often it’s that human-to-human encounter that eases the pressure and creates a sense of flow. If you detach yourself, you’re not going to get that. You’re starving yourself of the very thing that will nourish you.” Elton fears that medical schools have poor systems for identifying candidates whose emotional thermostat may prove all but impossible to adjust, or who simply lack the necessary resilience for the job.
She recalls running a workshop for senior faculty members of an Oxbridge medical school, where a clinician described an “academically brilliant” final-year student on placement in A&E who had needed his attendance form signed. The student had found his supervising consultant busy resuscitating a patient in cardiac arrest – and, quite undeterred, had literally waved the form under the consultant’s nose. To Elton’s astonishment, one of the faculty members, a medical school tutor, hearing this story pondered aloud: “Should I be worried about this student?”
“Duh! I mean, what is there not to be worried about when somebody has a decision tree: ‘Interrupt resuscitation, or don’t get my form signed’ and decides to interrupt the resuscitation? That person is not going to survive the complexity and messiness of the job.” Why wasn’t this instantly obvious to a medical school tutor? “Because the psychological component of what it takes to be a good doctor has sort of been excised.”
Too many trainee doctors realise too late they’re not cut out for the job. Many simply underestimate the commitment. The decision to train in medicine is made at 16, when students make their A-level choices. They are, Elton thinks, “really still just babies”. Secondary schools are liable to take any student who is good at science and assume a career in medicine is automatically a good idea. “They don’t have any understanding of what it’s actually going to be like, so they encourage pupils to apply. But if you’re very good at science and want to help people, being a doctor is not the only thing to do. The drugs, the technology – there have been people in labs who’ve done that work. You may not want them at your bedside, but you want brilliant brains doing that stuff. But schools don’t know about that.”
Too many trainee doctors realise too late they’re not cut out for the job. Many simply underestimate the commitment they’ve undertaken. “Something I don’t think people realise is how long this training takes. It’s mind-boggling.” The quickest route to qualification is to become a GP, which takes five postgraduate years. “But if you’re going to be a paediatric cardiologist it can be 12 years full-time – and then imagine if you’re doing that part-time.” Elton has lost count of the clients she has seen who want to quit but feel trapped by the fear of disappointing parents’ expectations.
“It’s a very noble profession. You are saving lives, and that is an amazing thing to be doing. Also, in this country there’s never been medical unemployment. So of course, there is incredible pride and pressure from young doctors’ families.” One client had “spent a staggering 15 years pursuing a career he never really enjoyed”; another had pushed himself for 10 years out of loyalty to his family, until severe panic attacks forced him to admit his real interest was actually elsewhere. Others had chosen the wrong specialty but felt stuck, the prospect of starting all over again in another discipline all but unthinkable. A study of obstetric trainees found a third regretted their choice; one of Elton’s clients had chosen oncology after her father died of cancer, only to have a traumatic experience on her very first day on a ward. The first patient looked exactly like her father; she promptly fainted at the foot of his bed.
More than half of medical students in the UK are now female, but Elton says the system has failed to adjust for this. “Nobody seems to have really thought about the fact, given the length of training, that the period which you’re trying to progress your training is the period in which you may also be hoping to have a family. Yet it’s so bloody obvious.” In a 2016 study of female trainee surgeons, one reported being repeatedly told, “You’re either a woman or a neurosurgeon, you can’t be both.” A neurosurgeon Elton counselled had been asked to edit an academic paper the day after her first child was born. When she said she couldn’t, her supervisor threatened to write to her research funders and “tell them about your lack of commitment. This will ruin your research career.”
The system is even less accommodating of doctors with health problems or disabilities, according to Elton. She cites the case of a medical student who was allowed to complete her medical degree after developing a visual impairment, only to be rejected for all foundation posts, without which she couldn’t progress to train in psychiatry, and eventually gave up and retrained as a teacher. “If you can’t stitch people up then you can’t go and be a surgeon. But if you want to be a psychiatrist you probably don’t need to stitch people up anyway.” A client applying to train as a GP was advised by her supervisor to lie on the forms, to conceal her diabetes, if she wanted to stand a chance of getting on to the course.
A prejudice against disability in the medical profession looks, on the face of it, baffling, but Elton has an explanation. “Just as doctors unconsciously position themselves in a separate category from the patients they treat, in order not to be overwhelmed by anxieties that they too could become sick,” she writes, so too do they “position themselves as ‘other’ than the disabled, in order to avoid confronting the possibility that they, too, might one day join their ranks”. In other words, “Doctors are supposed to be uber-able, not disabled.”
The picture Elton paints of chronic unhappiness, crippling anxiety and wasted talent makes me wonder how the NHS’s managers regard her. She no longer works in the NHS, but her view that the entire system by which we select, train and support doctors needs overhauling must be pretty confrontational. Is she considered an asset, or a nuisance? “I think both. I have some allies in quite senior roles in training different specialities who regard me as an asset. I’m sure there are others who think, ‘Oh that bloody Elton woman, bloody hell, I wish she’d shut up.’”
Elton warns that while our expectations of doctors become ever more unrealistic, the dangers of an inadequate support system put all of us at risk. She mentions the case of Dr Bawa-Garba, convicted of manslaughter following the death of a young boy in her care in 2011. The tragedy occurred on Bawa-Garba’s first day back on an acute ward following maternity leave; she’d been given no induction, the team was understaffed, and the computer systems failed. I spoke to a doctor just days after the GMC had successfully appealed to the high court in January to have Bawa-Garba struck off, and she told me she and all her colleagues were shocked by the news. If the system victimises and prosecutes doctors for mistakes made under impossible conditions, the doctor said, “There won’t be any doctors left by the time I’m old and need to be looked after. They’ll all have left.”
I ask Elton about another recent case of a doctor in court, this time for branding his initials on to livers during transplant surgery. “It’s such a terrible objectification of the patient,” she exclaims, looking dismayed. “I think it says something about power. In that moment you’ve got to psych yourself up, but that was somebody who psyched himself up a step beyond confidence, into omnipotence.” Delusions of omnipotence can be, she observes, just as dangerous as crises of confidence, but seldom recognised as such.
Interestingly, the best practice she ever came across in her work was in a hospice. The compassion and sensitivity displayed by one particular palliative care consultant was an object lesson in the dividend for patients of being treated by doctors with sound emotional wellbeing. I’m curious to know if she thinks it a coincidence that she found exemplary practice in a medical setting where staff knew they could do nothing to save lives. She considers the question carefully.
“I’ve seen some really, really burnt out, sour people working in hospices. So it’s not inevitable. But you can’t have the omnipotent defence, if you’re in a hospice, that you’re going to be on your white charger and zoom in and save lives. When you’re embracing the human condition, there has to be humility.”
‘Figure it out yourself, blue eyes’: an extract from Caroline Elton’s Also Human
Hilary, a GP, came to see me because she was thinking about leaving medicine. “I’ve reached the end of the road with general practice,” she explained. Like many other GP clients, Hilary told me that she felt present-day general practice pulls doctors in opposing directions. On the one hand, she lived in fear of incorrectly reassuring a patient that a particular symptom didn’t warrant a referral to a specialist for further investigation. On the other, she dreaded being singled out by her clinical managers as having an inappropriately high referral rate to specialist services. Damned if you do and damned if you don’t.It was five years since Hilary had qualified as a GP, but even before she finished her training, she had started to doubt whether it was the right career for her. “I’m not a natural doctor,” she said. “I constantly feel like a square peg in a round hole.”
I asked Hilary to tell me about her first job as a doctor. She described how her heart sank when she saw from her rota that she’d been placed on the on-call team on her first day. This meant that, in addition to her responsibilities on the surgical ward to which she had been attached, she also had to assess new patients as they were admitted to the hospital for surgery. It’s a bit like trying to be in two places at once; nobody wants to be on call on day one.
On her first morning, she was immediately informed by the senior nurse on the surgical ward that, following surgery, one of the patients urgently needed to be seen by a doctor. Naively, Hilary asked which other doctors were available.
“Mr Baker, the surgical consultant, is on a course, Mr Shah, the registrar, is on annual leave and Dr Glover is off having worked a bunch of nights. It’s just you,” the nurse said.
The nurse led Hilary to the patient’s bedside. The first thing Hilary clocked was the patient’s strange, grey pallor. With extreme difficulty, the patient opened her eyes and whispered: “Doctor, am I going to die?” Then, a second later, a barely audible request: “Doctor, please call my family.”
‘Is there another doctor here?’ the junior asked, finding it hard to believe she was expected to fly solo
Hilary didn’t have a clue whether the patient was at death’s door, or whether she should summon the family; she also didn’t know whether there were medical interventions she should be making to save the patient’s life. Moving away from the patient’s bedside to confer with the nurse, Hilary asked for help.
“You’re going to have to get used to this,” the nurse told her. “Mr Baker never turns down an opportunity to operate. With some of the patients on this ward, it might have been better if they had escaped the knife. They’re often even sicker when they come out of theatre.”
A junior nursing assistant called the senior nurse away. Left on her own and unsure what to do next, Hilary decided to review the patient’s notes. There were no clues there, either. With mounting anxiety, she wondered whether she should call the registrar from another team, or ask the senior nurse to come back. Nothing that she had learned in medical school had prepared her for this situation.
By chance, Fiona, a fledgling doctor attached to another ward, walked down the corridor and caught sight of a panic-stricken Hilary.
“Are you OK?” she asked.
“Not really,” Hilary replied.
She led Fiona to the patient’s bedside; neither of them spoke as they peered down at the sickly looking patient, who had fallen asleep again.
“I’ll call my mum,” Fiona whispered.
Hilary thought Fiona was joking.
“Mum’s a nurse on the rapid-response team,” Fiona explained. “She’ll know what to do, and I am sure she will come if I ask.”
Fiona’s mother appeared five minutes later. She took one look at the patient, realised she was desperately unwell and called the consultant anaesthetist. A couple of minutes later, the anaesthetist appeared, agreed with his nursing colleague’s opinion and, less than 10 minutes after that, the patient was transferred to the high-dependency unit for urgent medical treatment.
The patient survived. And Hilary’s first day continued.
All the time that Hilary had been trying to sort out the desperately ill patient, her bleep had been going off, summoning her to the surgical assessment unit (SAU). As soon as the patient was transferred, she dashed down to the SAU and encountered an extremely angry nurse. “There are nine patients waiting. Where have you been?”
Before Hilary had the opportunity to explain, the nurse gave a rushed account of each of the nine patients whose names were on the whiteboard. Hilary absorbed almost nothing.
“Is there another doctor here?” she asked, finding it hard to believe that she was expected to fly solo on the SAU as well as on the ward.
“Emergency admission. Everyone’s in theatre,” was the unwelcome response. The nine names on the whiteboard were swimming in front of Hilary’s eyes. She was desperate to know if any of the names were higher priority than the others. “Could you possibly help me work out who I should see first?” Hilary asked.
“Figure it out yourself, blue eyes,” the nurse replied. And, with that, she walked off – probably to get on with her own enormous list of tasks.
A huge number of experiences brought me to my belief that the NHS doesn’t care. That it chews people up, spits them out
Over a decade had passed when Hilary told me about her day one, but she could still remember the face and name of the desperately ill patient. She could still recall that sense of panic and fear. I asked if she thought there was any relationship between her horrendous first day and her current feelings about her work; she told me she couldn’t see a link.The following day, Hilary emailed me: “I was thinking yesterday about your question. On reflection, I think that my first day was just the beginning of a huge number of experiences (of myself and others) that brought me to my current belief on working within NHS medicine. That it just doesn’t care. That it chews people up, spits them out and then gets another well-meaning chump to replace them. Sorry if that sounds harsh, and I do have some sadness in writing it, but I also think it’s 100% true.”
It would be reassuring to think that Hilary’s experience was exceptional. Sadly, this is not the case. In the UK, all first-year doctors start work on the same day – the first Wednesday in August. Hilary’s conclusion was that her experience was, in fact, commonplace. “Lots of my F1 [first year] colleagues had similar experiences,” she told me. “And the following year, in a completely different hospital, the same thing happened to the F1 on my new team. That day, I had induction in the morning into my new role as an F2, and got to the wards only in the early afternoon. But the new F1 in the team had been left to firefight all morning. It happens all the time.”
Hilary’s conclusion is borne out by studies of first-year foundation doctors. A 2014 programme of research commissioned by the GMC reached the following conclusions: “The August transition was highlighted where F1s felt unprepared, particularly for the step-change in responsibility, workload, degree of multitasking and understanding where to go for help.” The study also emphasised how pressures on the healthcare system can affect recent medical graduates: “Trainees may feel prepared for situations when all goes to plan, but unprepared when exposed to high volumes of work which demand prioritisation and multitasking; or uncertain thresholds [not knowing when to refer to seniors]; inadequate team-working; or when seniors are not easily accessible.”
In 2009, a group of researchers at Imperial College in London found that, across England, in-hospital mortality was significantly higher in the week following the first Wednesday in August than in the previous week.
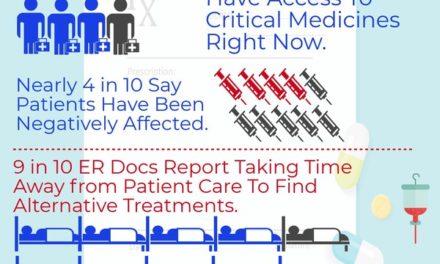
In 2011, an online survey reported that 90% of physicians in the UK felt that the August transition had a significant negative impact on patient care. Respondents highlighted the inadequacy of measures at local level to support junior staff in their induction, and to ensure patient safety. The title of the paper was August Is Always A Nightmare, taken from a comment by one of the physicians in the survey. August is the cruellest month, it seems, at least for patients in teaching hospitals in the UK.
What strikes me most forcefully about Hilary’s story is that the whole set-up seems so precarious. Given that day one is a national fixture across the whole country, why was the supervising consultant away on a course? The registrar should not have been allowed to go on annual leave at the same time. What if the patient had died and Hilary had been held responsible? Back-up provision should have been made on the surgical assessment unit in case all the experienced staff had to rush into theatre to deal with an emergency. Do we really want a system where a patient’s life depends on someone’s mother arriving in time?
All names have been changed